
Introduction
Diabetes mellitus (DM) is one of the leading noncommu-nicable chronic diseases and represents a growing chal-lenge for public health worldwide. It is estimated that approximately 537 million adults aged 20 to 79 years are living with the disease globally, a figure that may reach 783 million by 2045 due to population aging and changes in lifestyle patterns [1]. In Brazil, the crude prevalence of diag-nosed diabetes in 2019 was 7.7% (7.4–8.0), representing a relative increase of 24% compared with the prevalence observed in 2013 [2].
In 2023, approximately 30 million diabetes-related visits were recorded in primary health care units across the coun-try, highlighting the high demand for continuous and spe-cialized care [3]. The management of DM is complex due to the presence of multiple associated comorbidities. Nota-bly, cardiovascular diseases (CVD) [4], myocardial infarc-tion (MI) [5] and stroke (AVC) [6], stand out as the leading causes of mortality in this population [7].
In addition, microvascular complications such as diabetic retinopathy, nephropathy, and peripheral neuropathy are prevalent and have a substantial impact on patients’ qual-ity of life [8–10]. Furthermore, the coexistence of arterial hypertension, dyslipidemia, and obesity exacerbates cardio-vascular and metabolic risk, requiring integrated and multi-disciplinary approaches [11, 12].
Thus, beyond its high prevalence, DM exhibits sub-stantial clinical, genetic, and socioeconomic heterogene-ity, affecting populations with diverse risk profiles, disease trajectories, and therapeutic responses [13, 14]. This under-scores the need to develop specific patterns of complica-tion burden across population subgroups [15, 16]. Accurate stratification of these profiles is essential to inform clinical decision-making contributing to hypothesis generation for future multidimensional phenotyping approaches. Within this context, investigating the population groups most affected by DM is imperative.
Accordingly, the present study aims to identify patterns of complication burden among individuals with diabetes mellitus based on sociodemographic, behavioral, and clini-cal characteristics, and to examine their co-occurrence with diabetes-related comorbidities.
Methods
Study design
This is a cross-sectional study conducted during a Diabetes Health Campaign in a city in southern Bahia, aimed at pro-viding multidisciplinary care to patients with diabetes affili-ated with the Brazilian Unified Health System (SUS).
Participants and data collection
Individuals with a prior diagnosis of DM, aged 18 years or older, residing in the city where the campaign was conducted and receiving care through the Unified Health System (SUS) were included. Participant recruitment was conducted through convenience sampling, including direct invitation by researchers and dissemination via media. Therefore, the sample reflects individuals voluntarily attending a health campaign and does not represent a population-based sam-pling frame. As a convenience sample, it may overrepresent individuals who are more health-conscious, symptomatic, or with more advanced disease, limiting the generalizability of the findings.
Data collection was performed by medical and nurs-ing students who were appropriately trained and super-vised by health professionals. Participants completed standardized clinical and epidemiological questionnaires. In addition, they underwent ophthalmologic examination, including pupil dilation and retinography, for detailed reti-nal assessment.
Pre-analytical variables were also evaluated, including fundoscopic examination results (presence or absence of retinographic abnormalities), diabetic retinopathy (present or absent), presence of established diabetic nephropathy, medical history, smoking status, medication use (insulin, oral antidiabetic agents, or other medications). Neurological disease was defined based on self-reported medical diagno-sis of neurological conditions (excluding diabetic peripheral neuropathy, which was assessed separately through protec-tive sensation testing). Clinical evaluation included assess-ment of ulceration, amputation, posterior tibial (PT) and dorsalis pedis (DP) pulses, and protective sensation.
Statistical analysis
To identify clusters of patients with similar characteristics, latent class analysis (LCA) was applied. The included indi-cators were selected based on clinical relevance and their potential to distinguish patterns of complication burden within the screened population. In LCA, variables should meaningfully contribute to class separation rather than introduce redundant information; therefore, indicator selec-tion prioritized constructs that captured complementary aspects of peripheral impairment [17].
Models specifying one to four latent classes were esti-mated using maximum likelihood via the expectation– maximization (EM) algorithm. Model selection followed principles of parsimony, statistical adequacy, and substan-tive interpretability [18]. Fit was evaluated using log-likeli-hood values, Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), likelihood-based goodness-of-fit statistic (G2 ), and entropy. Because AIC applies a lighter penalty for model complexity and may favor overparam-eterized solutions, greater weight was given to BIC for class enumeration. Lower values of AIC, BIC, and G2 were inter-preted as indicating improved fit after accounting for model complexity. Entropy was examined as a measure of clas-sification precision but was not used as the primary deter-minant of the number of classes [19].The average posterior probabilities (AvePP) for class membership were examined to assess classification quality. High mean posterior prob-abilities indicate adequate separation between classes and support the reliability of modal assignment for descriptive purposes.
To formally compare nested solutions, the Vuong–Lo–Mendell–Rubin (VLMR) and Lo–Mendell–Rubin adjusted likelihood ratio tests were conducted. The comparison between the one- and two-class models was statistically significant (p<0.001), indicating that a homogeneous (sin-gle-class) model was insufficient to represent the data struc-ture. Although the two- versus three-class comparison also reached statistical significance (p<0.01), the three-class solution generated a very small class (2.1% of the sample) and yielded a higher BIC compared with the two-class model. Considering parsimony, convergence stability, and interpretability, the two-class solution was retained for sub-sequent analyses.
All models were estimated in R (version 4.5.0) using the poLCA package. To reduce the risk of local maxima, each model was estimated using multiple random starting values (n=50 replications), and convergence was verified through replication of the maximum log-likelihood across runs.
Individuals were assigned to latent classes based on the highest posterior probability (modal assignment). Subse-quently, Prevalence ratios (PR) and 95% confidence inter-vals were estimated using Poisson regression models with robust variance estimators, adjusted for age and sex, given the cross-sectional design and the non-rare frequency of outcomes. Analyses were conducted in R (packages poLCA, ggplot2, and cowplot) and Stata (version 12).
Ethical aspects
As this study involved human participants, the ethical stan-dards established by Resolution No. 466/12 and its com-plementary guidelines were fully observed. The project to which these data are linked, entitled “Evaluation of the main complications observed in diabetic patients treated at the Diabetes Health Campaign in Itabuna, Bahia,” was duly submitted to and approved by the Research Ethics Commit-tee, under Opinion No. 5779758/2022.
Results
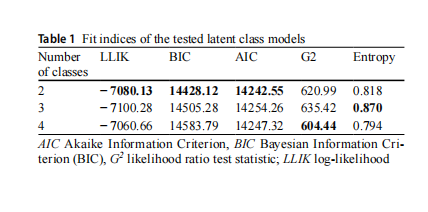
A total of 1,542 individuals were evaluated, with a mean age of approximately 62 years (±11.76), ranging from 18 to 101 years. Females predominated (64.66%), and most participants had completed elementary education (50.48%). Regarding clinical characteristics, the mean duration of DM was approximately 10 years, and 21.89% of participants used insulin. To examine different patterns of complication burden, three latent class models were constructed with two, three, and four classes (Table 1).
Model selection considered AIC, BIC, G2 , log-likeli-hood, and entropy. Although the 4-class model presented lower AIC and G2 values and the 3-class model showed higher entropy, the 2-class model yielded the lowest BIC. In latent class modeling, criteria that impose stronger penal-ties for model complexity, such as BIC, are often preferred to reduce the risk of overfitting and to favor more parsi-monious and stable solutions. Moreover, model selection in LCA should balance statistical fit with substantive interpret-ability and theoretical coherence. Additionally, although the VLMR and LMR tests indicated statistical improvement for the 3-class solution (p<0.01), the additional class comprised only 2.1% of the sample and did not substantially improve BIC compared to the 2-class model. Given the small class size and the higher BIC value, the 2-class solution was retained based on parsimony and stability considerations.
The mean posterior probabilities for class membership were high for both classes (Class 1 (AvePP=0.85); Class 2 (AvePP=0.91), indicating good classification precision and clear separation between latent profiles.
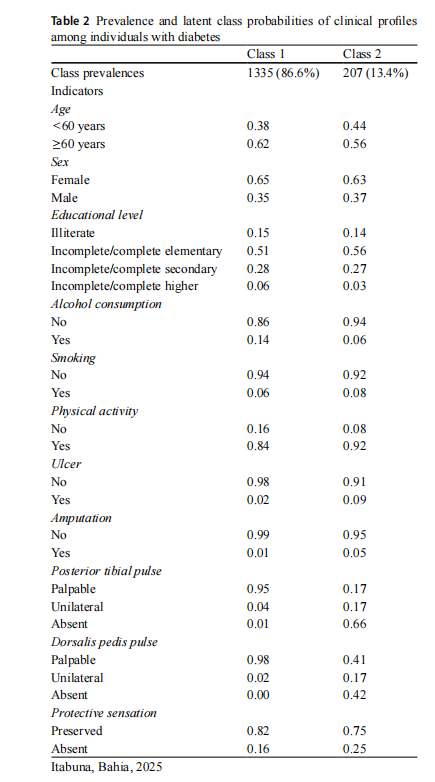
Thus, the two classes consisted of three sociodemo-graphic indicators (i.e., age, sex, and educational level), three lifestyle indicators (i.e., alcohol consumption, smok-ing, and physical activity), and five indicators related to foot health assessment (i.e., ulceration; amputation; PT and DP pulses; and protective sensation).
Class 1 comprised 86.6% of the evaluated individuals and showed higher probabilities of including those aged 60 years or older (0.62), female (0.65), with incomplete or complete elementary education (0.51), non–alcohol con-sumers (0.86) and non-smokers (0.94), physically active (0.84), without ulcers (0.98) or amputations (0.99), with PT (0.95) and DP pulses (0.98), and preserved protective sen-sation (0.82). Class 2 represented 13.4% of the individuals and followed a pattern similar to that of Class 1; however, it presented higher probabilities of smoking (0.08), presence of ulcers (0.09) or amputations (0.05), absent PT (0.66) and DP pulses (0.42), and impaired protective sensation (0.25) (Table 2).
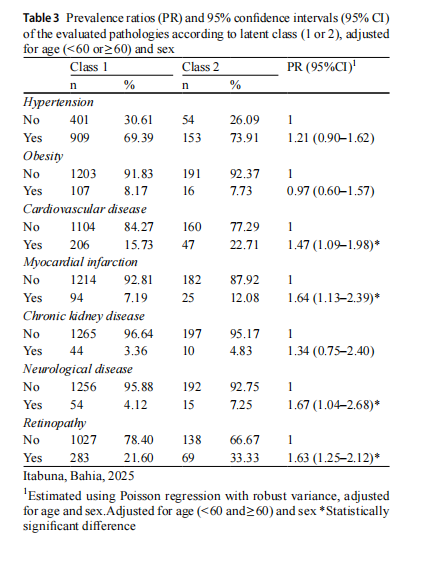
Given the increased prevalence of certain indicators in Class 2, this group was identified as having a higher complication burden in the current study. Accordingly, associated pathologies were examined, individuals in Class 2 exhibited a higher co-occurrence of cardiovascu-lar diseases (PR=1.47; [95% CI 1.09–1.97]), myocardial infarction (PR=1.61; [95% CI 1.11–2.34]), neurological disease (PR=1.63; [95% CI 1.03–2.61]), and retinopathy (PR=1.65; [95% CI 1.27–2.15]) (Table 3).
Discussion
This study identified two latent classes among individuals with diabetes, reflecting distinct levels of complication bur-den within a screening population. The class with a higher burden was primarily characterized by indicators of periph-eral vascular and neuropathic impairment, including ulcer-ation, amputation, absent posterior tibial and dorsalis pedis pulses, and impaired protective sensation. Individuals in this class also showed a higher prevalence of cardiovascu-lar disease, myocardial infarction, neurological disease, and retinopathy. In contrast, the lower-burden class showed a predominance of preserved vascular and sensory function.
These findings indicate that the identified classes primar-ily represent a gradient of peripheral complication burden rather than comprehensive multidimensional clinical phe-notypes. The structure of the model was largely driven by foot-related clinical indicators, which capture advanced manifestations of vascular and neuropathic impairment, reflecting heterogeneity in complication burden among individuals with diabetes [20]. In this context, its contri-bution lies in describing how complication burden is orga-nized, rather than redefining established clinical categories or supporting individual-level clinical decisions [21, 22]. This approach may contribute to resource allocation and population-level planning, particularly in complex chronic conditions such as DM [23, 24]. However, its applicability at the individual level remains to be established.
The higher complication burden class showed a greater co-occurrence of cardiovascular disease, myocardial infarc-tion, neurological disease, and retinopathy. Given the over-lap between class-defining indicators and these outcomes, particularly in relation to vascular impairment, these asso-ciations are clinically expected and should be interpreted as patterns of co-occurrence rather than independent relation-ships. Considering the cross-sectional design, these findings do not imply causal or prognostic associations, but instead reflect the simultaneous presence of multiple complications in individuals with more advanced disease [25, 26].
From a population health perspective, the identification of a subgroup with a higher burden of complications within a campaign-based screening context contributes to under-standing how complex clinical manifestations aggregate in real-world settings. These findings are descriptive and should be interpreted as complementary to existing clinical frameworks, without direct implications for individualized therapeutic decision-making.
The co-occurrence of vascular, neuropathic, and micro-vascular complications observed in the higher burden class is consistent with the known clustering of advanced diabe-tes-related complications, with an increased risk of plantar ulcers, infections, and nontraumatic amputations [27–31].
Some limitations should be considered. The cross-sec-tional design precludes establishing temporal relationships between class-defining indicators and associated comorbid-ities. The higher burden class likely represents individuals with more advanced or cumulative disease manifestations, rather than a group at increased prospective risk. Addition-ally, the classes were influenced by peripheral complication indicators, particularly foot-related variables, and did not include key metabolic parameters such as glycemic control, lipid profile, or blood pressure. This limits interpretation as a comprehensive cardiometabolic phenotype. Finally, class assignment was based on modal posterior probabilities without three-step correction, which may introduce classifi-cation error and potential bias in associations with external variables [32].
Future research should evaluate the generalizability of these patterns across diverse populations and incorporate longitudinal designs and broader clinical indicators to assess their stability and potential relevance in different contexts.
Funding The Article Processing Charge (APC) for the publication of this research was funded by the Coordenação de Aperfeiçoamen-to de Pessoal de Nível Superior - Brasil (CAPES) (ROR identifier: 00x0ma614).
Declarations
Conflict of interest The authors declare that they have no known com-peting financial interests or personal relationships that could have ap-peared to influence the work reported in this paper.
Open Access
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.o rg/licenses/by/4.0/.
This article is excerpted from the 《Acta Diabetologica》 by Wound World.
