Introduction
The most prevalent form of monogenic diabetes is GCK-hyperglycaemia, where heterozygous loss-of-function variants in the GCK gene (encoding glucokinase) impede glucose sensing, leading to an isolated mildly raised glycae-mic set-point that generally does not necessitate treatment or diabetes complication surveillance. Pregnancy is a spe-cial situation where insulin therapy may be used to mitigate macrosomia in an unaffected fetus. Despite the unequivo-cal value to individuals, families and healthcare systems in diagnosing GCK-hyperglycaemia, >80% of monogenic diabetes cases remain undiagnosed [1].
In genetic testing, the American College of Medical Genetics and Genomics (ACMG) framework is used to classify identified variants as: benign, likely benign, vari-ant of uncertain significance (VUS), likely pathogenic (LP) or pathogenic (P), with P/LP variants considered to be clinically actionable positive results and VUS regarded as inconclusive/negative results [2]. Classification is based on fulfilment of certain combinations of pathogenic vs. benign criteria of different strengths of certainty. One rea-son for missing a diagnosis of monogenic diabetes is when genetic testing only demonstrates a VUS with insufficient evidence to classify the variant as pathogenic (i.e., caus-ative of hyperglycaemia). In VUS reclassification studies in other heritable conditions, most VUS remain as VUS or are downgraded to a benign classification [3]. Noting the recent development of international variant classification guide-lines specific to GCK by The Clinical Genome (ClinGen) Resource, we reviewed all GCK VUS in a cohort of indi-viduals with suspected monogenic diabetes to determine the rate and direction of VUS reclassification.
Methods
We aimed to assess the utility of reanalysing GCK vari-ants of uncertain significance (VUS) as an intervention to improve the detection of monogenic diabetes.
We searched genetic testing records in the SA Pathol-ogy Genetics & Molecular Pathology Laboratory in Ade-laide, Australia to collate all previously identified VUS in GCK. Each VUS was then reviewed according to the Clin-Gen Monogenic Diabetes Variant Curation Expert Panel (VCEP) Specifications to the ACMG/AMP Variant Inter-pretation Guidelines for GCK Version 1.3.0 (https://cspec.genome.network/cspec/ui/svi/doc/GN086) as outlined in Table 1. Various combinations of specifications permit a VUS to be upgraded to LP classification, e.g., 2 moderate and ≥2 supporting criteria. Some specifications pertain to variant-specific information available online (e.g., genomic population databases), whilst other specifications pertain to patient-level data which were obtained through medical record review. Each specification has a standard level of evi-dence which may be upgraded or downgraded if additional criteria are fulfilled– e.g., a supporting ‘PP’ criterion may be upgraded to moderate in accordance with set rules, thereby making it a ‘PP_moderate’ criterion.
The study was ethically approved by Central Adelaide Local Health Network Human Research Ethics Committee (HREC Ref no. 2021/HRE00232). Individuals with VUS that were upgradable to LP classifications were contacted to provide counselling regarding their newly positive genetic test results, and concurrently consented for study participa-tion. The HREC waived the need for study consent in indi-viduals whose VUS remained as VUS as patient re-contact was not otherwise required in these cases and only audit-level data are provided herein.
Results
We identified eight individuals (age at testing 12–43 year,six females, two males) with previously identified GCK VUS on monogenic diabetes next generation sequencing (NGS) gene panel testing. Variant types comprised: four single nucleotide substitutions resulting in missense vari-ants, one in-frame 3 bp deletion resulting in a single amino acid deletion, two small intronic variants, and one large multi-exon duplication, which is the first reported case of a duplication involving GCK [4]. Variant reclassification is outlined in Table 2, and comparisons between study cura-tions and original curations are depicted in Table 3.
Individual pathogenicity criteria
Wherever the PM2 criterion (absent from controls) was applied in the original classification, we downgraded the criterion from moderate to supporting (i.e., ‘PM2_support-ing’) in line with GCK VCEP recommendations (Table 3).
Three other pathogenicity criteria were modified or newly applied at moderate strength. The most common newly applied criterion was the PP4 criterion (specific phe-notype), which was based on review of pre-existing glyco-haemoglobin, blood glucose and pancreatic autoantibody results, with a moderate level of evidence achieved in each applicable case. By the GCK VCEP guidelines, the PP4_ moderate criterion is applicable when an individual has an HbA1c of 5.6–7.6% (38–60 mmol/mol) (maximum value used if multiple results) AND fasting glucose 5.5–8 mmol/L (100–144 mg/dL) AND the presence of an additional fea-ture of GCK-hyperglycaemia as outlined in Table 1 (e.g., negative pancreatic autoantibodies, oral glucose tolerance
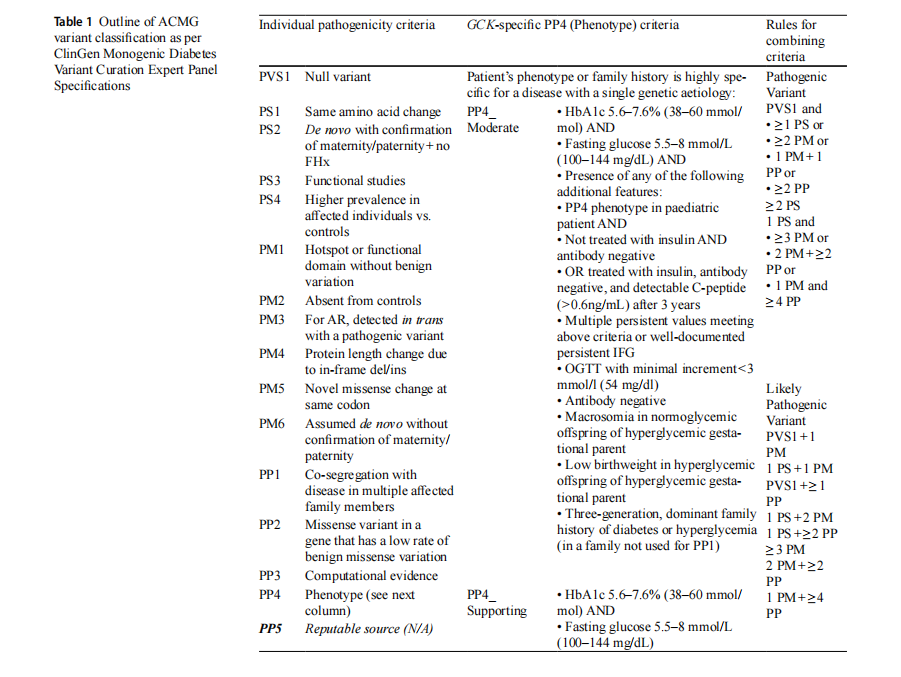
test with minimal increment<3 mmol/l (54 mg/dl) etc.). If only HbA1c and fasting glucose criteria are met with-out additional GCK-hyperglycaemia features, then PP4 is applicable at its usual supporting level of pathogenicity. In our cohort, PP4 had only been applied in 1/8 original clas-sifications (Case 5), and only at a supporting level of evi-dence, in a case where the referring clinician specified that the phenotype was suspicious of GCK-hyperglycaemia. On variant review for the study, we were able to apply PP4 in this case and an additional 5 cases by extracting patient data and appraising it against the GCK VCEP specifications for PP4. In each of these 6 cases, there was evidence to fulfil the moderate version of the PP4 criterion based on HbA1c 5.6–7.6%, fasting glucose 5.5–8 mmol/L and negative pan-creatic autoantibodies.
Another newly applied criterion of moderate strength was the moderate version of the PS4 criterion (prevalence in affected individuals vs. controls), which was fulfilled in Case 5 based on the finding of the variant in published literature (3 occurrences) and another Australian laboratory (1 occurrence). As the PS4_moderate criterion requires 4–6 occurrences of a variant in affected unrelated individuals, the other Australian laboratory observation of this variant was essential to achieve this pathogenicity criterion. It was identifiable due to an entry in the Shariant database, which is an online platform that shares variant interpretations and associated evidence between Australian clinical genetic testing laboratories [5].
The remaining newly applied criterion of moderate strength was PM1 (altered protein length), applied to the multi-exon GCK duplication. RNA studies were attempted in this case to secure the higher level pathogenicity cri-terion of PS3 (in vivo/in vitro functional study). Reverse transcriptase-PCR (RT-PCR) using a fresh blood sample from the patient indicated tandem duplication of exons 3–6, resulting in a frameshift and premature termination codon, but the level of mRNA expression in blood did not meet the quality threshold for this assay and was therefore not
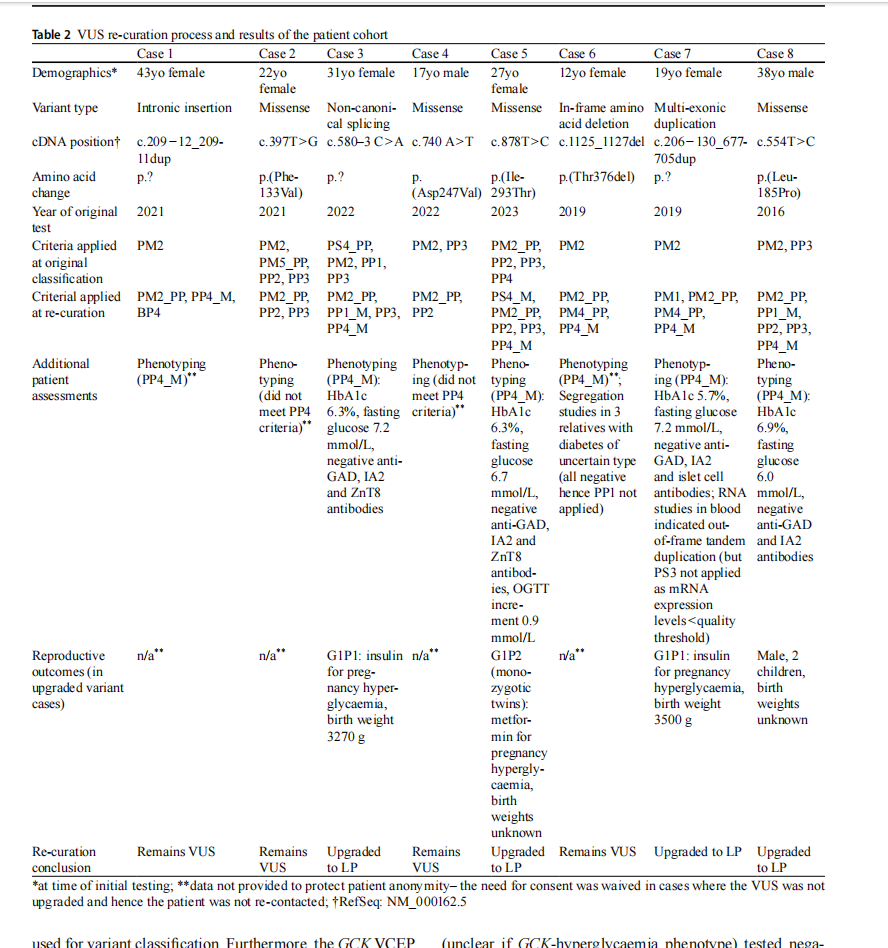
used for variant classification. Furthermore, the GCK VCEP specifications preclude the use of patient cell lines in RNA evidence, with the presumption that there might be a differ-ent occult variant in the individual that is causing aberrant splicing rather than the variant in question.
Segregation studies were attempted to achieve the PP1 criterion in Case 6 but all available relatives with diabetes (unclear if GCK-hyperglycaemia phenotype) tested nega-tive for the proband’s VUS.
Overall variant classification
Ultimately, we were able to upgrade 4/8 (50%) VUS (i.e., uninformative genetic test results) to an LP classification
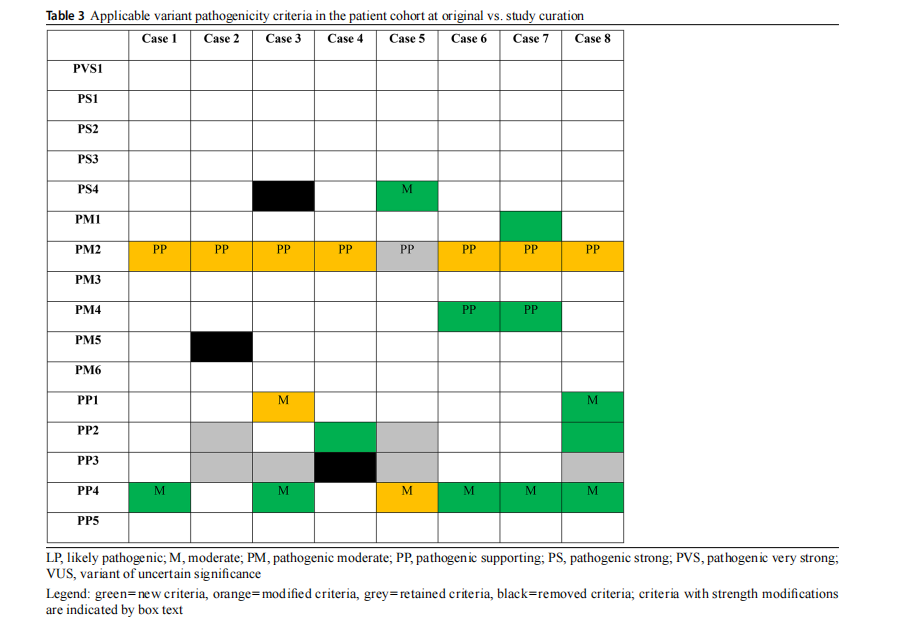
(i.e., positive results). This comprised 4/6 cases with the PP4_moderate criterion (including Case 5 with the PS4_ moderate criterion and Case 7 with the PM1 criterion), whilst the other 2/6 cases had insufficient additional criteria to reach LP classification. Cascade testing of relatives with hyperglycaemia is currently underway.
Discussion
To our knowledge, this is the first VUS reclassification study in monogenic diabetes using the ClinGen gene-specific framework. We achieved a high rate (50%) of VUS reclas-sification to positive results without the need for additional tests. Two prior studies utilising the generic ACMG variant classification guidelines with intensive functional experi-ments also achieved high rates of VUS reclassification in the monogenic diabetes setting, but with a substantially greater burden of investigation that is unfeasible in routine prac-tice [6, 7]. The high VUS upgrade rates of 50–74% between these monogenic diabetes studies far exceed rates in non-diabetes conditions [3, 8, 9]. Why there is a higher yield of VUS reclassification in diabetes is uncertain but may relate to endocrine genes being less studied than other conditions (e.g., cancer, deafness), resulting in a greater burden of true disease-causing variants classified as VUS due to a lack of previous observations in the literature/patient databases that would permit pathogenic classification.
The pathogenicity criterion of greatest utility in VUS reclassification was a clinical phenotype specific for GCK-hyperglycaemia, emphasising the importance of referring clinicians carefully assessing the patient’s glycaemic his-tory to evaluate the pre-test probability of finding a LP/P GCK variant and providing this information on request forms to aid the genetic testing laboratory in variant clas-sification. Based on our experience in the current study, we recommend noting HbA1c, fasting blood glucose and either antibody negativity or a small oral glucose toler-ance test (OGTT) increment as a feasible minimum dataset to achieve the phenotype criterion at a moderate degree of pathogenicity. Detailed phenotyping to the strength required for a moderate pathogenicity criterion for other genes that currently do not have gene-specific VCEP guidance may be facilitated by multidisciplinary variant review boards with involvement of the treating clinician and reporting labora-tory [10]. In Australia, the EndoGen National Endocrine Genetics Network holds regular national multidisciplinary team meetings involving endocrinologists, clinical geneti-cists, genetic counsellors, genetic pathologists and genetic scientists, and multiple VUS reclassifications have been achieved through this forum.
Another useful pathogenicity criterion was comparing the rate of the variant in affected individuals vs. healthy controls. This may be achieved by inter-laboratory liaison, most efficiently via centralised databases (e.g., the Austra-lian Shariant database) that facilitate case and variant clas-sification sharing between participating laboratories [5].
VUS that potentially affect splicing are particularly dif-ficult to assess. In general terms, aberrant splicing may be elucidated through RNA studies; however, GCK is poorly expressed in blood, making it difficult to perform RNA expression studies using blood samples. Furthermore, the GCK VCEP specifications explicitly exclude RNA studies from patient cell lines from being used as a strong patho-genicity criterion due to the possibility that the resultant splicing may relate to other unidentified genomic variation. A supporting criterion based on in silico prediction of aber-rant splicing may instead be used; this was used to support pathogenicity for one intronic variant with a maximum Spl-iceAI score>0.2 (Case 3) and to support ‘benignity’ of the other intronic variant with SpliceAI scores<0.2 (Case 1). An alternative approach is to perform in vitro functional splicing assays via a minigene construct after prioritisation of putative splicing variants using in silico models [7]; how-ever, this is a labour-intensive process that is generally not feasible in individual patient care.
How VUS are managed is of increasing importance given the rise of gene panel testing which expectedly produces a greater burden of VUS than single gene sequencing. The use of gene-specific guidelines should, as in the present study, bring clarity to many variants otherwise considered to be of uncertain significance. This may be of particular value in individuals where gene panel testing reveals variants in multiple genes. Lucchesi et al. described one such kindred where dual variants were found in GCK and HNF1A, with the GCK variant ultimately classified as pathogenic and the HNF1A classified as a VUS through ClinGen Monogenic Diabetes Expert Panel guidance in conjunction with the family’s phenotype compatible with GCK-hyperglycaemia [11].
Aside from unresolved VUS, another potential cause of a false-negative genetic test result in individuals with monogenic diabetes is missed copy number variants (CNV). These variants typically necessitate dedicated copy number analysis to be performed, either via whole exome sequenc-ing (WES)-based CNV-calling bioinformatic pipelines as routinely employed in our laboratory [12], or via multi-plex ligation-dependent probe amplification (MLPA) [13]. Our cohort includes the first reported duplication involving GCK. By contrast, multiple partial or whole GCK deletions have been previously reported. As highlighted in a report by Yu et al., GCK deletions may be missed not only by Sanger sequencing but also by WES unless dedicated CNV detec- tion using WES data is pursued [13]. These cases emphasise the importance of considering CNVs– including duplica-tions– in the assessment of suspected monogenic diabetes.
The major limitation of our study is its small size. We acknowledge that the ClinGen VCEP that created the GCK-specific guidelines is charged with systematic consensus review of monogenic diabetes gene variants for pathogenic-ity and submission to the ClinVar database. This is an ongo-ing consolidated program of variant reanalysis by many internationally recognised experts that will clarify the patho-genicity of a vast number of VUS in the coming years. Our present work is complementary to the aims of the ClinGen VCEP in its immediate, real-world application of the GCK-specific VCEP guidelines, which has already resulted in the revision of our patients’ diagnoses to GCK-hyperglycaemia. This study, albeit small, should raise awareness amongst local laboratories of the option of immediate VUS reanaly-sis using the GCK-specific VCEP guidelines. For treating clinicians, this study highlights the utility of VUS reanaly-sis in the diagnostic work-up of individual patients and the importance of collating the required patient-level data. The timing of VUS reanalysis is especially important in repro-ductive age women given the significant impact on man-agement from a diagnosis of GCK-hyperglycaemia rather than gestational diabetes. Noting that many ClinGen VCEPs exist at various levels of progress across the specialty of clinical genetics, clinicians and laboratories should rou-tinely consider, at least, the option of reanalysis of reported VUS rather than waiting for VCEP outcomes which will understandably take time given the complexity of the task and may not examine the particular VUS in question. Addi-tionally, although desirable, local laboratories may not nec-essarily have a mechanism by which to flag VUS that have been upgraded by a VCEP and so clinician request for VUS reanalysis remains an important clinical tool for patients in the community.
In conclusion, this study confirms the utility of VUS reclassification using gene-specific VCEP guidelines in monogenic diabetes. Readily available biochemical pheno-typing data were instrumental in reclassification, whilst the more intensive processes of RNA studies and segregation studies performed here were not directly additive. How we assess GCK variants will be of increasing importance given recent recommendations for more widespread GCK test-ing e.g., in all non-obese women with gestational diabetes [14]. The 50% rate of upgraded VUS is especially striking given that a diagnosis of GCK-hyperglycaemia typically allows cessation of diabetes treatment and surveillance. Pending further studies, there may be a cost-effectiveness argument for routine GCK VUS reclassification with careful biochemical phenotyping to avoid ongoing costs of unnec-essary diabetes care. Looking forward, clinicians should ideally provide the relevant biochemical data to laborato-ries at the time of genetic test requesting to allow accurate upfront variant classification and avoid the burden of VUS for patients, clinicians and laboratories.
Acknowledgements We thank A. Dubowsky for performing RT-PCR studies in Case 7, and all clinicians involved in clinical care of the reported patients, including S. Stranks, T. Thynne and J. Chemmanam.
Author contributions SD, JP and HS were involved in the conception, design, and conduct of the study and the analysis and interpretation of the results. All authors reviewed variant re-curations. KW performed segregation studies. JP and AW constructed the tables. SD wrote the first draft of the manuscript, and all authors edited, reviewed, and ap-proved the final version of the manuscript. SD is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data
Funding Open Access funding enabled and organized by CAUL and its Member Institutions. SD is the recipient of the Royal Adelaide Hos-pital Mary Overton Early Career Research Fellowship, the Royal Aus-tralasian College of Physicians Fellows Research Establishment Fel-lowship, and the Endocrine Society of Australia Postdoctoral Award.
Data availability Restrictions apply to the availability of data gener-ated and analysed during this study to preserve patient confidentiality. The corresponding author will on request detail the restrictions and any conditions under which access to some data may be provided.
Declarations
Conflict of interest The authors have no relevant conflict of interest to disclose.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.o rg/licenses/by/4.0/.
This article is excerpted from the 《Acta Diabetologica》 by Wound World.
