
伤口世界
电子邮件地址: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
- 星期五, 30 1月 2026
Medical Treatment of Lung Cancer: Can Immune Cells Predict the Response? A Systematic Review
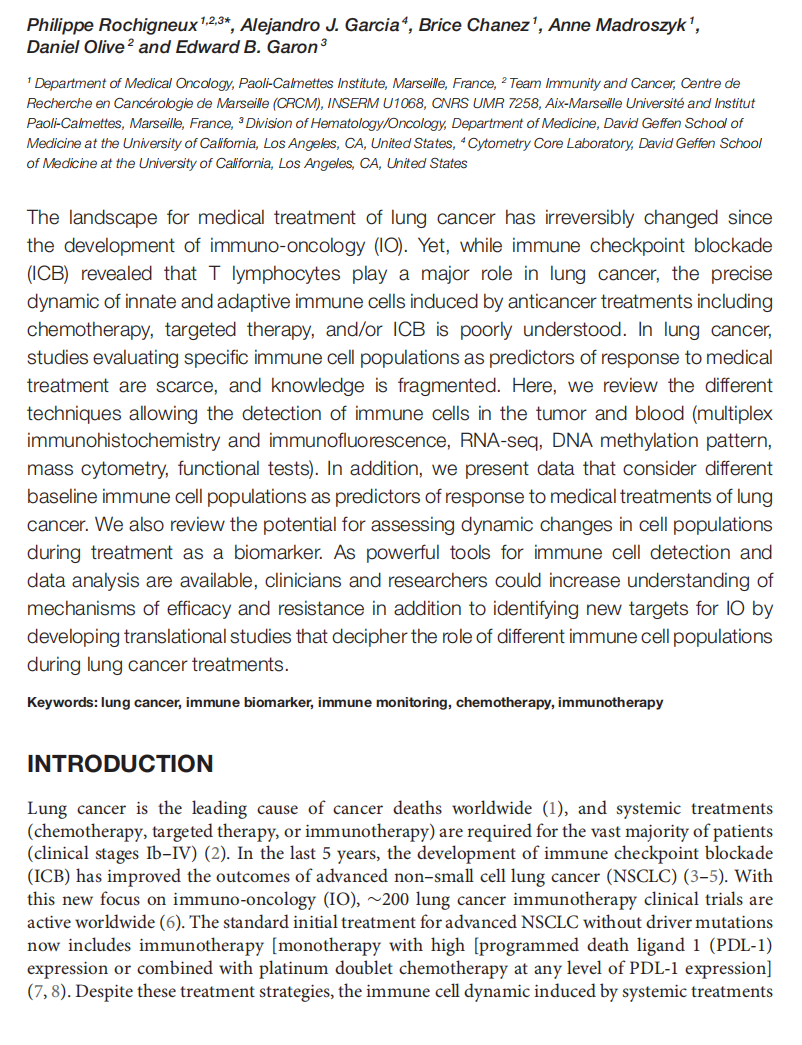




This article is excerpted from the《Frontiers in Oncology》by Wound World
- 星期四, 29 1月 2026
Comparing real-world outcomes of total neoadjuvant treatment and CRT at a tertiary medical center
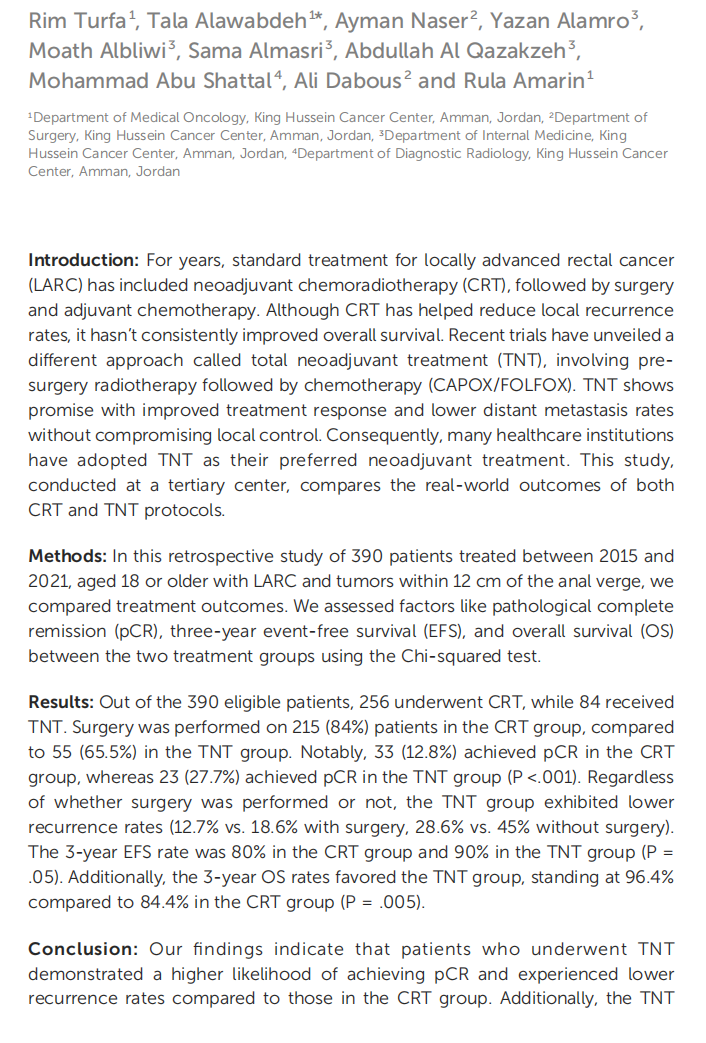

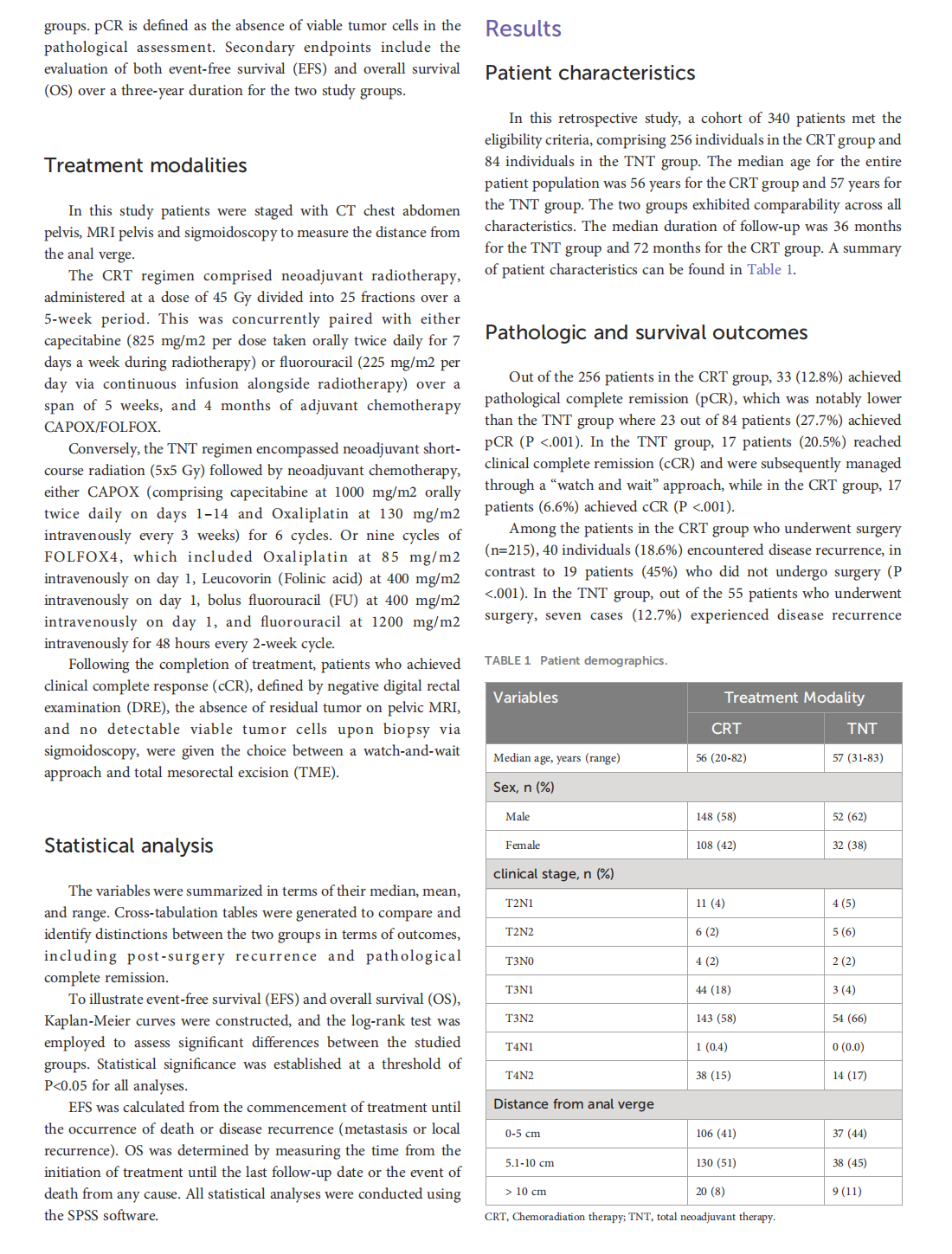
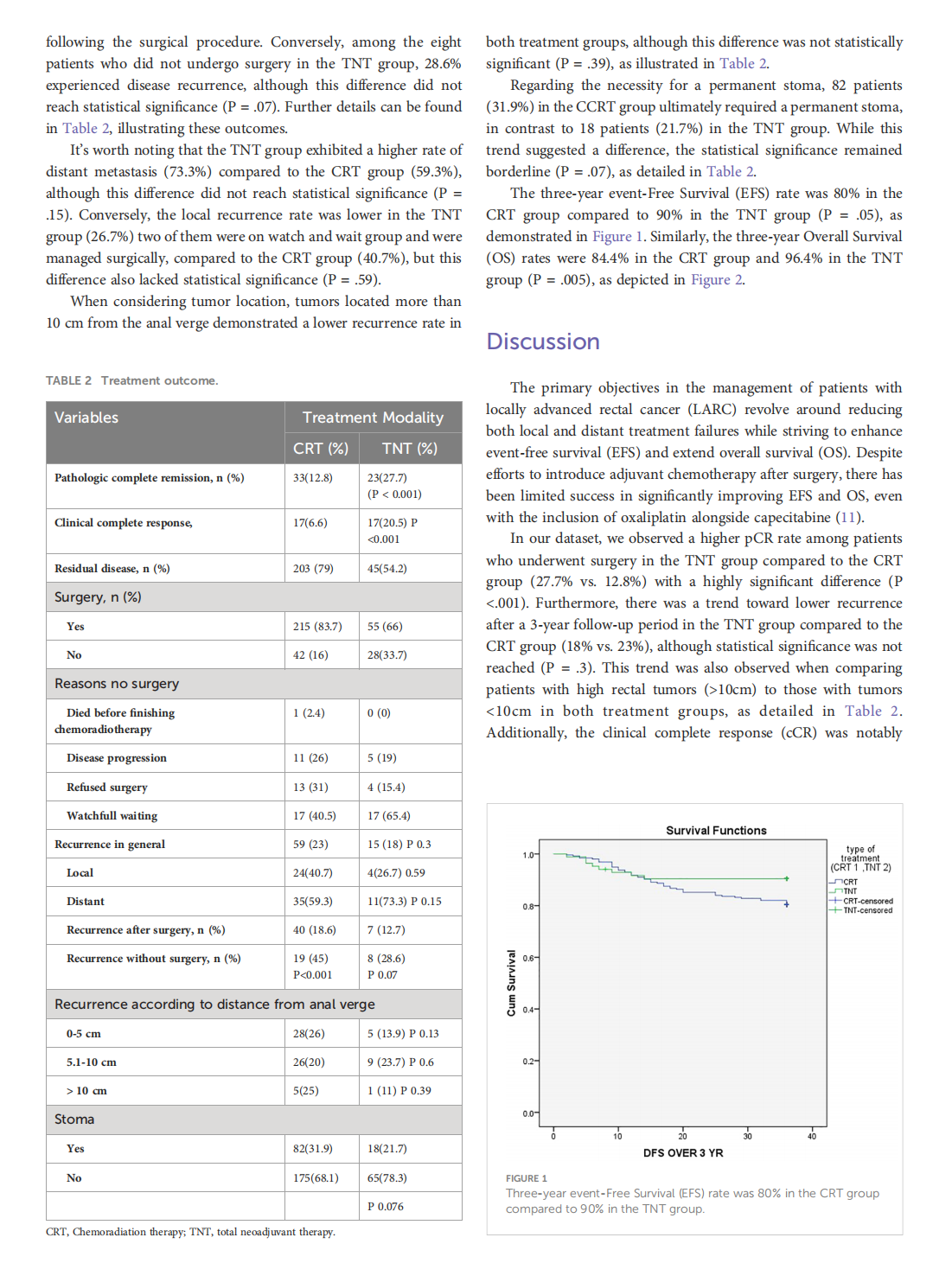


This article is excerpted from the《Frontiers in Oncology》by Wound World

- 星期三, 28 1月 2026
Benefits of Surgical Over Medical Treatment for Unilateral Primary Aldosteronism




This article is excerpted from the《Frontiers in Endocrinology》by Wound World

- 星期二, 27 1月 2026
Treatment Utilization and Medical Problems in a Community Sample of Adult Women With Anorexia Nervosa
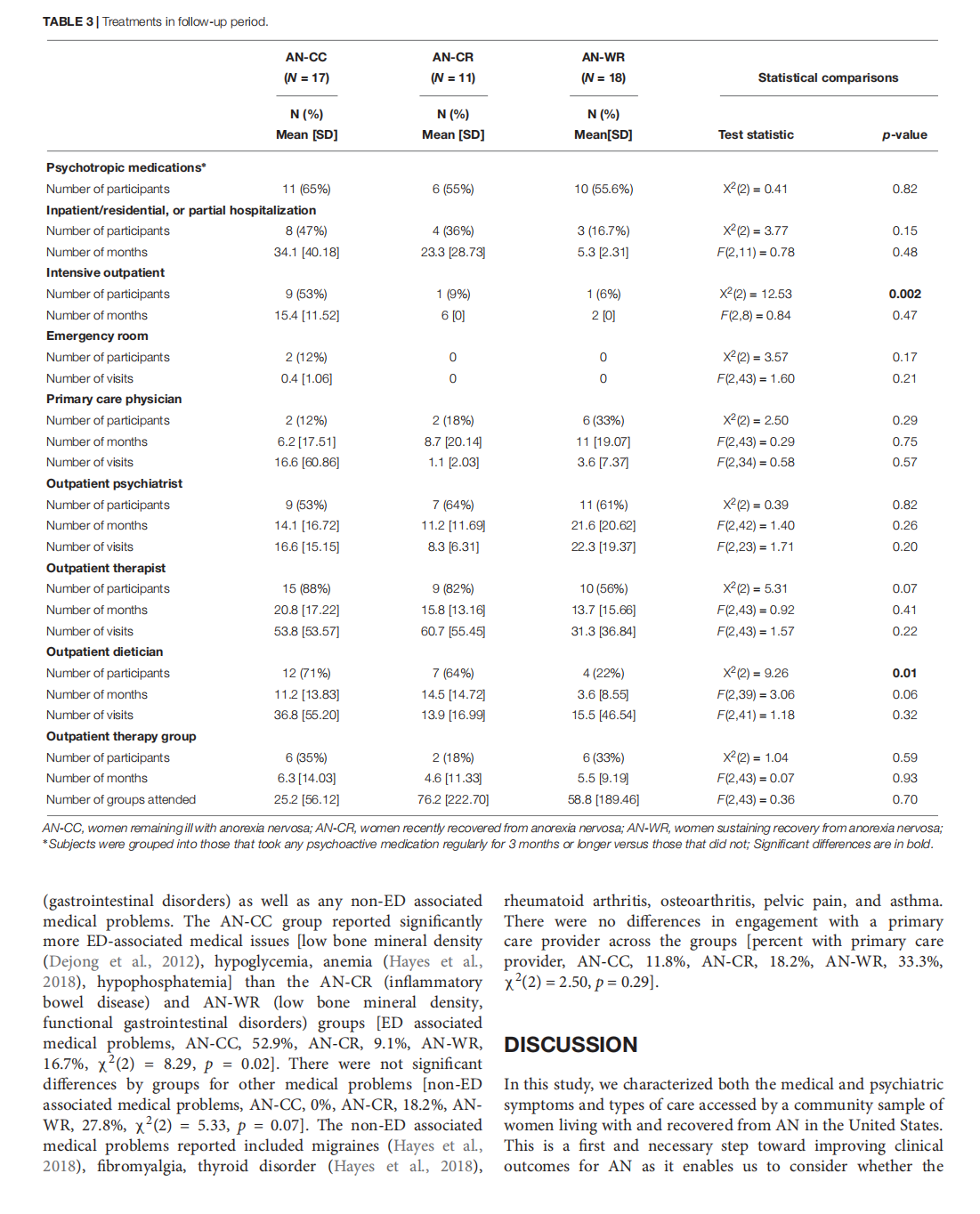


This article is excerpted from the《Frontiers in Psychology》by Wound World
- 星期一, 26 1月 2026
Implantable biomedical materials for treatment of bone infection

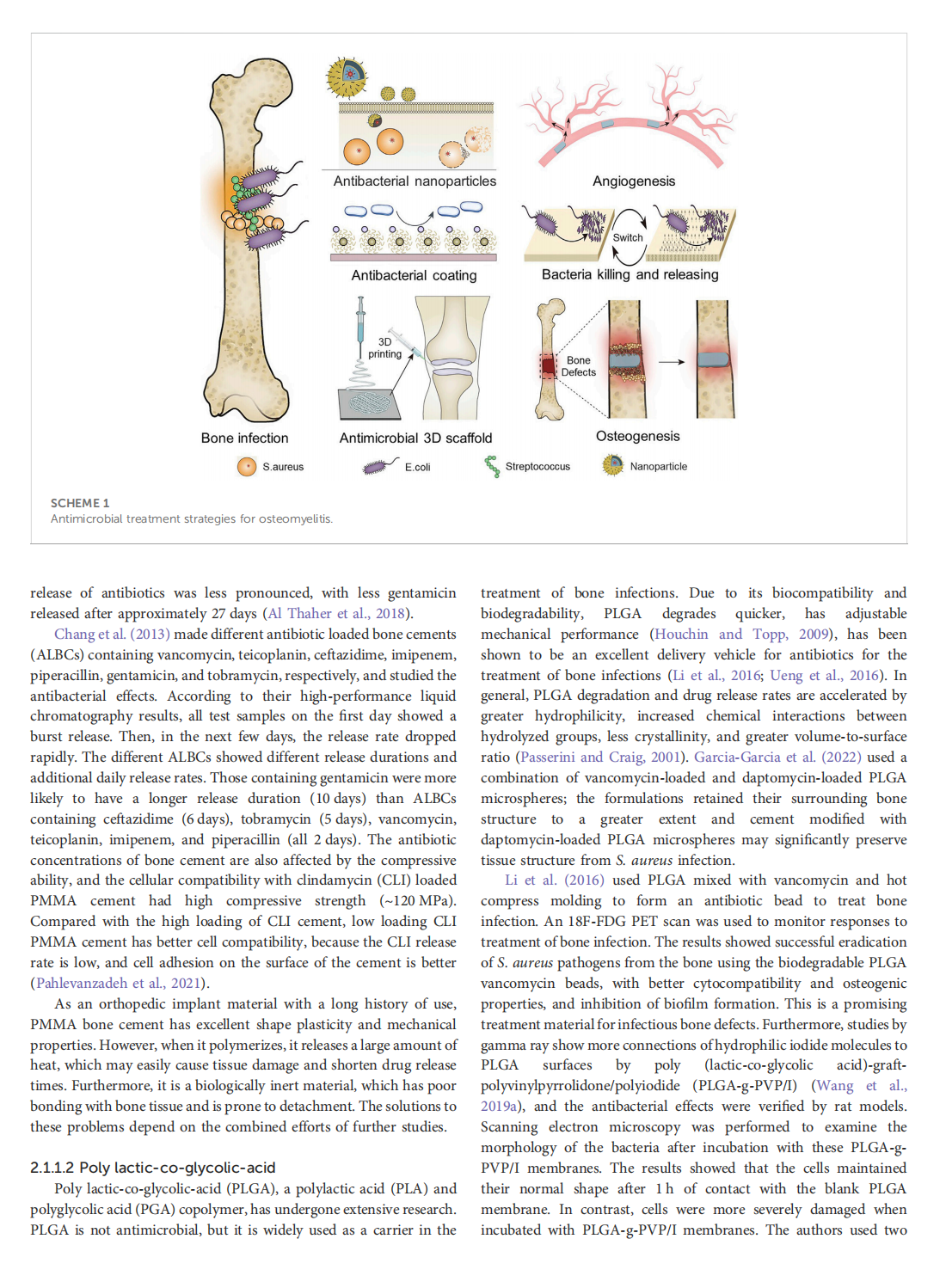
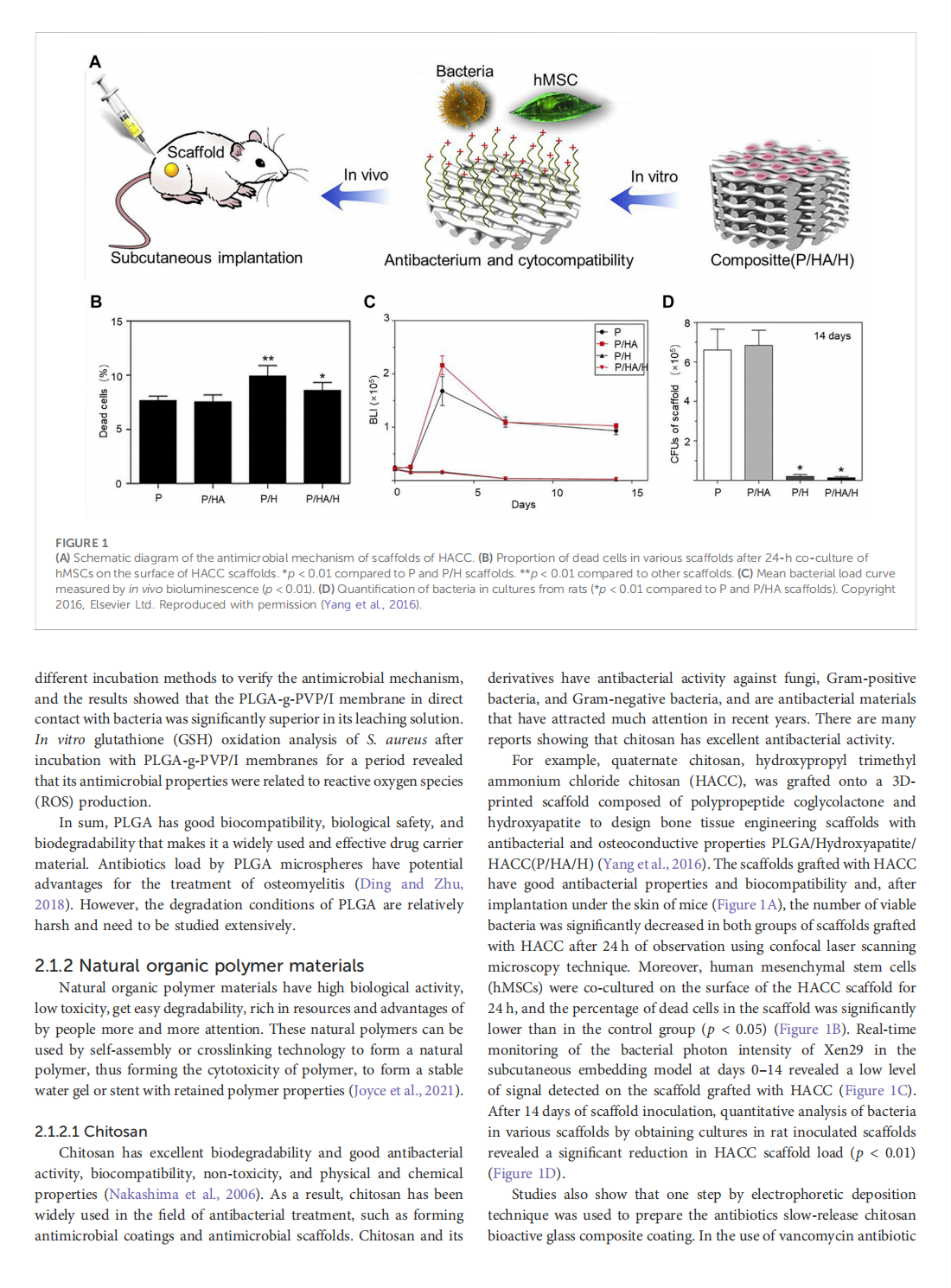
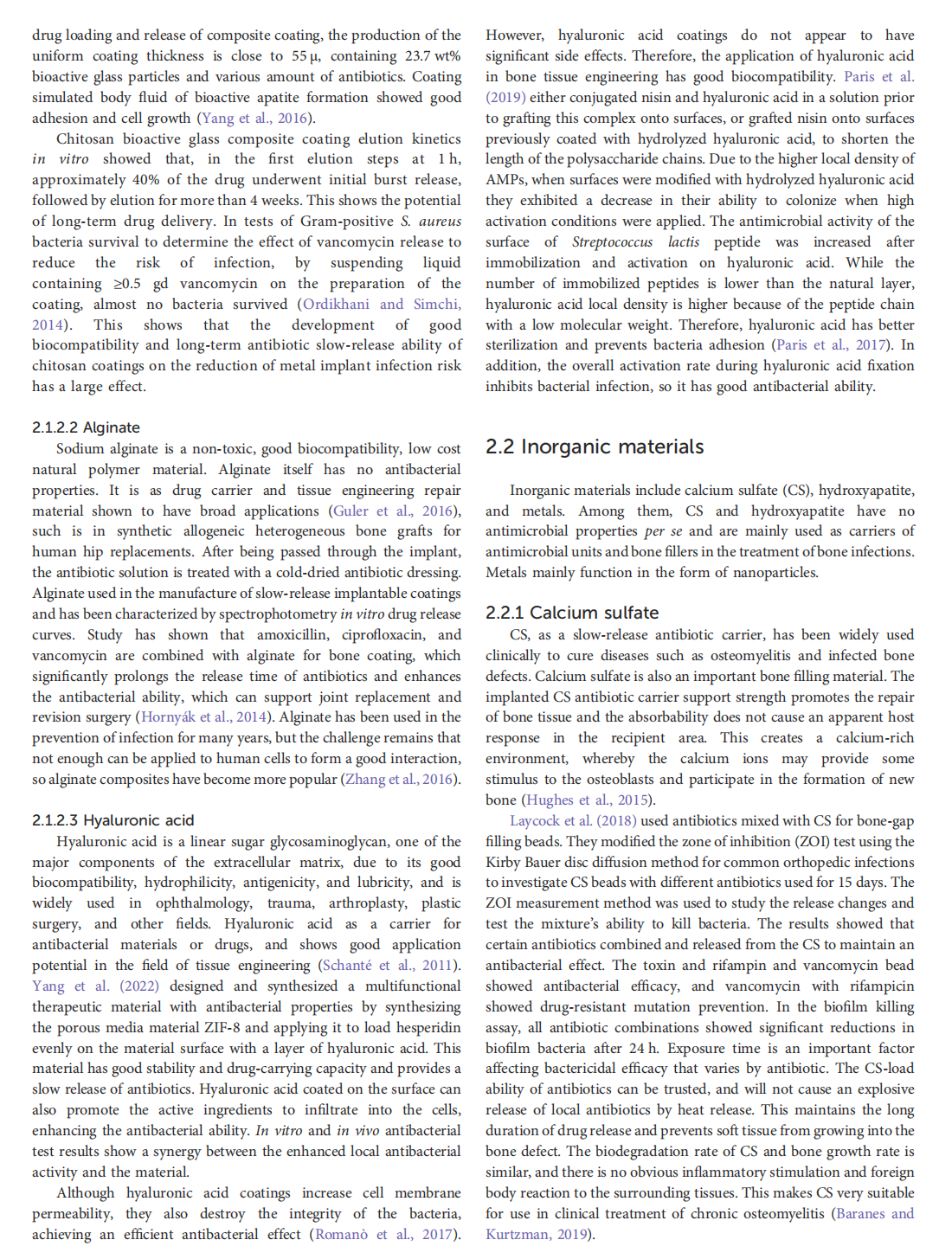

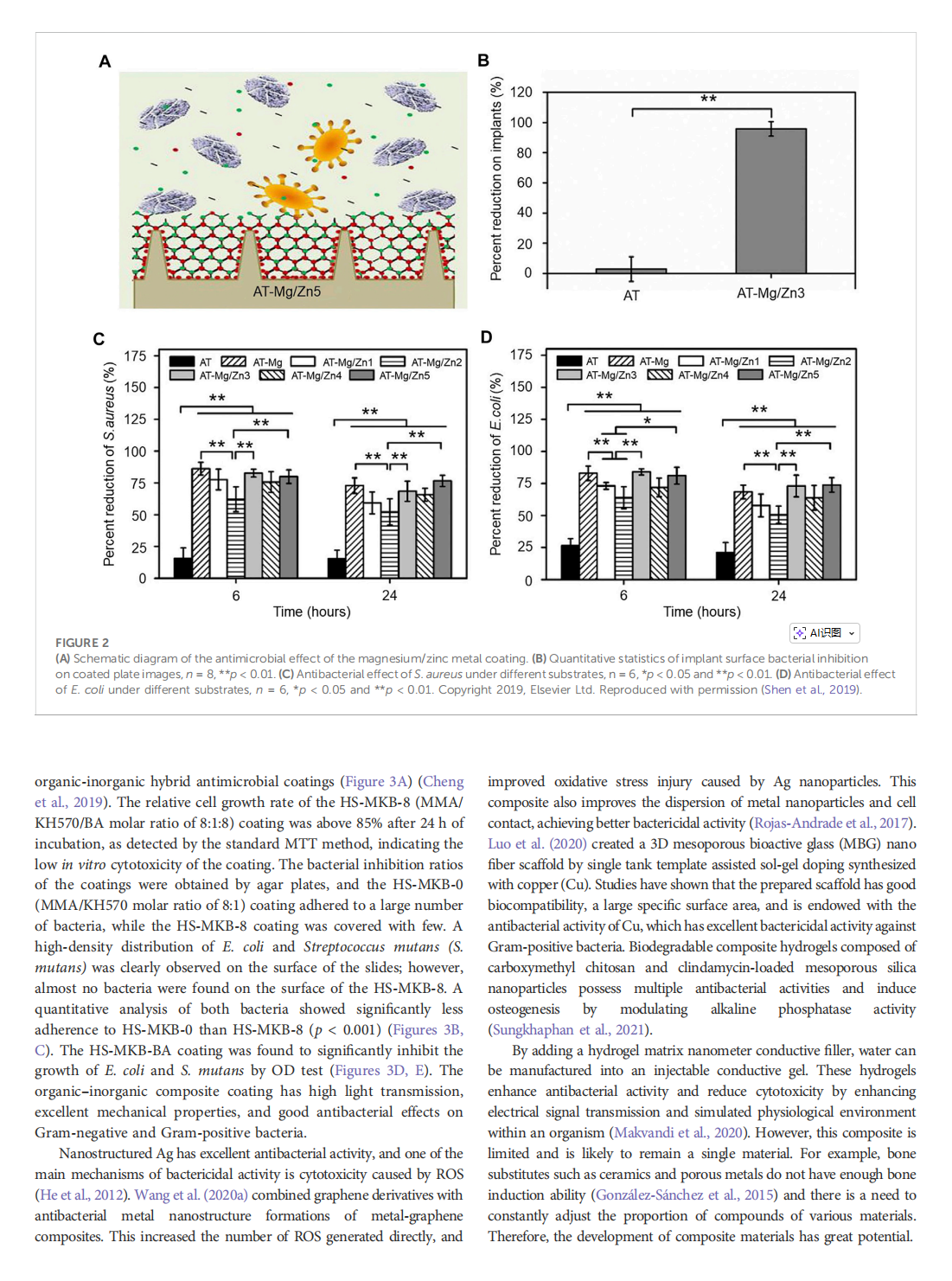






This article is excerpted from the《Frontiers in Bioengineering and Biotechnology》by Wound World
- 星期五, 23 1月 2026
Editorial: Best surgical treatment of breast cancer managed primarily with neoadjuvant medical therapy
This article is excerpted from the《Frontiers in Surgery》by Wound World

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}