
1、Introduction
Performance measurement in long-term care is a challenge of growing importance as the population ages and the demand for longterm care services increases [1]. There is increased interest in international benchmarking of the quality of long-term care services provided in different healthcare systems, as it has considerable potential to improve patient outcomes [2]. International benchmarking is essential to signal differences between countries and can enhance learning across countries by exploring the reasons behind the differences. International benchmarking has been used effectively in other areas, such as acute care [3]. Some proposals for indicators in long-term care with potential for international comparisons have been published recently [2,4]. However, they require considerable data collection capabilities, which many countries do not have at the moment [5].
An alternative approach for comparisons of performance of longterm care facilities across countries is to take advantage of existing performance measurement initiatives. In such an approach the central question is whether the data being collected by different performance measurement initiatives produce comparable rates. The Organization for Economic Cooperation and Development (OECD), an international organization of mostly high- and middle-income countries, recently used such an approach to publish data on pressure ulcer prevalence in longterm care facilities [3].
Comparing indicator rates, collected through different performance measurement initiatives, is generally undesirable, as actual differences in performance are likely to be skewed by differences in measurement methodologies [6]. At the same time, the establishment of internationally coordinated multi-country performance measurement initiatives with a broad inclusion of countries is difficult to achieve [7]. Starting with existing performance measurement initiatives and modifying them if necessary to enhance comparability, might have a higher likelihood of success.
Pressure ulcers in long-term care facilities are a strong candidate for internationally comparable measurements. Pressure ulcer indicators are among the most frequently used measures of the quality of care provided in long-term care settings [8,9]. A high level of international standardization of definitions of pressure ulcers has been achieved based on expert consensus [10]. This suggests an increased likelihood that independent pressure ulcer measurement systems could produce comparable results. Considering the existing wide use of pressure ulcer indicators and the relative homogeneity of measurement, pressure ulcers indicators have been chosen as the focus of our analysis.
In order to calculate performance indicators, such as pressure ulcer rates, long-term care facilities’ resident level data may be collected via different approaches. Two approaches prevail in high- and middleincome countries: one involves a cross-sectional ad hoc survey that is repeated periodically and produces point prevalence measures. The other approach involves using data collected continuously by long-term care facilities to monitor the well being of residents. A notable example of the latter approach is the Resident Assessment Instrument/Minimum Data Set [5,11,12]. Currently this instrument is only used in a few countries [5] and an international common minimum dataset in long-term care is still not widely established [13]. Hence the most promising approach to obtaining internationally comparable performance data in long-term care in the short run is based on point prevalence survey initiatives, on which our study focuses.
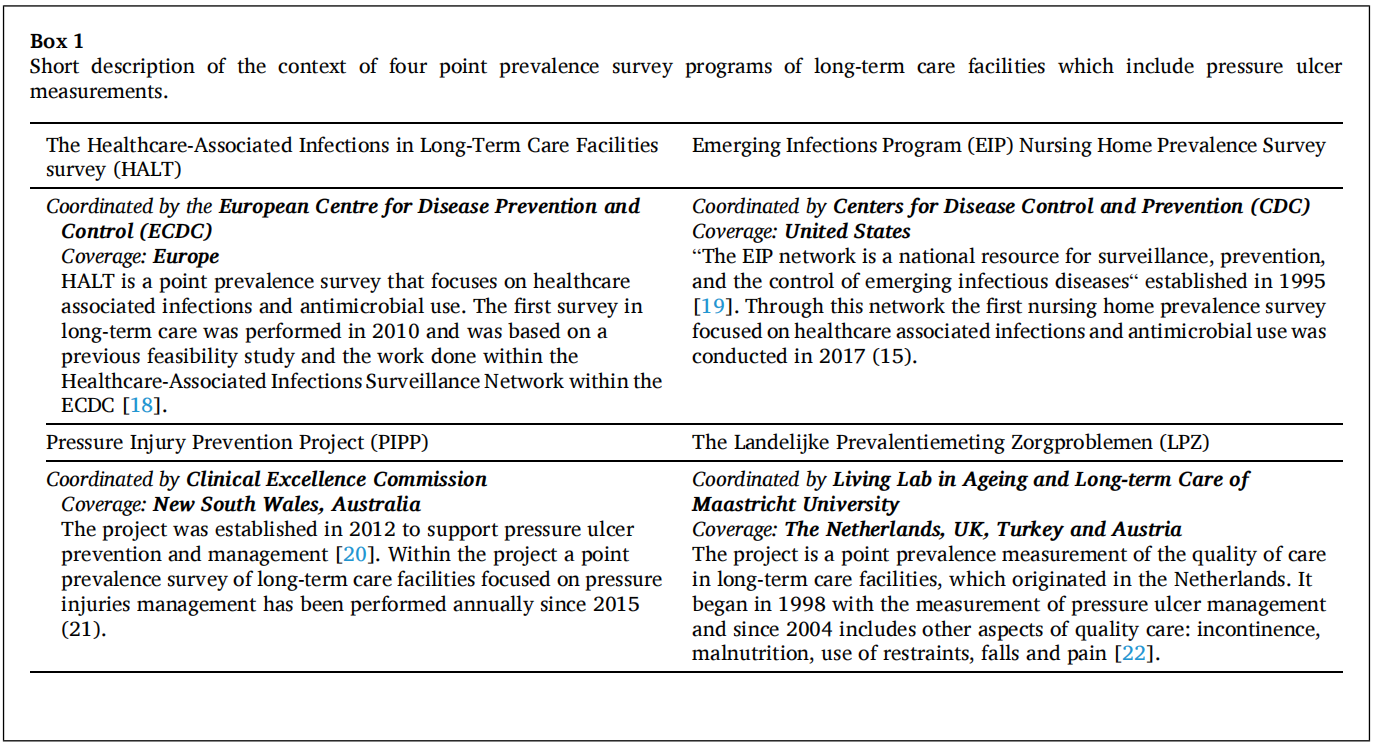
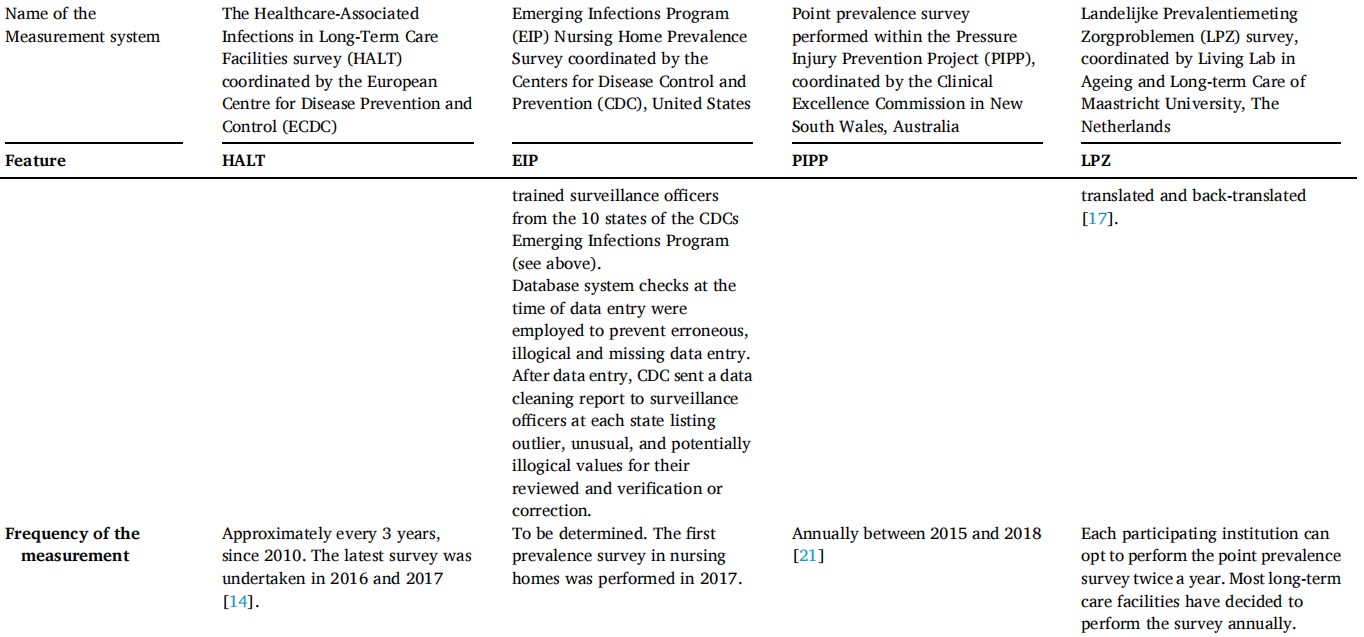
We identified four point prevalence survey programs which includedata on pressure ulcer prevalence in long-term care facilities (Box 1)from 28 high- and middle-income countries spanning three continents: the Healthcare-Associated Infections in Long-Term Care Facilities (HALT) survey, coordinated by the European Centre for Disease Prevention and Control (ECDC) [14], the Nursing Home Prevalence Survey undertaken within the Centers for Disease Control and Prevention (CDC) Emerging Infections Program (EIP) in the United States [15], the point prevalence survey performed within the Pressure Injury Prevention Project (PIPP), coordinated by the Clinical Excellence Commission in New South Wales, Australia [16], and the Landelijke Prevalentiemeting Zorgproblemen (LPZ) survey, coordinated by the Living Lab in Ageing and Long-term Care of Maastricht University in the Netherlands [17].
This paper aims to identify possible avenues for international comparisons of data on pressure ulcer prevalence among residents of longterm care facilities by comparing and analyzing these four point prevalence measurement systems. More specifically, this study aims to answer the questions:
• What are the key methodological features of the four point prevalence measurement systems?
• To what extent do these measurement systems have the ability to adhere to a common set of methodological criteria to facilitate international comparisons of the prevalence of pressure ulcers in long term care facilities?
2、Materials and methods
2.1 Choice of pressure ulcer measurement systems
The four point prevalence measurement systems analyzed represent a convenience sample of point prevalence measurement initiatives of pressure ulcers in long-term care facilities. The specific choice of these four systems was guided by a number of considerations. All four systems have been established as a program to be repeated over time, as opposed to being a one-time evaluations. The programmatic nature of the measurement systems is important to confirm that they can be sustained in time and hence could be used as a standing instrument allowing international comparisons. Two of the initiatives (EIP and PIPP) are limited to single countries, while the other two are multi-country initiatives. The implication is that the assessment will include comparisons of subnational, national, and multi-country initiatives. The geographic spread of the included initiatives means that all three regions and countries (Europe, United States, and the Pacific area) represented by the organizations that published the international guideline on pressure ulcers in 2019 [10] are included in the analysis.
2.2 Analysis of the measurement systems
A descriptive analysis was performed to outline key features of the point prevalence measurement systems. The description follows a list of items developed by reviewing the literature. In particular, we considered published criteria for indicator selection [6,23,24], important methodological features for international comparisons [25,26] and challenges specific to pressure ulcer measurement [27–30].
The list of items used to describe the point prevalence measurement systems are grouped around three high level issues: the breadth of the measurement system, its accuracy, and the structures in place to support the data collection process. These issues and the items within them have been selected taking into account the specific purpose of this analysis, i.e. using existing measurement systems for international comparisons. Items describing the breadth of the four initiatives were considered important to give a sense of their scope and likely scalability. Items related to the accuracy of the four point prevalence systems inform the expected validity and reliability of the measurements. The items used to describe the supporting structures are potential indicators of the ease with which features of data collection methodologies of each point prevalence system can be modified. Such modifications may be necessary to adapt to an internationally agreed common set of methodological criteria.
In addition to describing the key features of the four point prevalence survey programs, we also considered whether the pressure ulcer prevalence rates obtained from these surveys could produce comparable rates. To compare results from different point prevalence surveys, they must share key methodological specifications. These specifications do not necessarily signal a methodology of superior or inferior quality, but need to be consistent among the surveys to be able to provide comparable results. The set of reference specifications against which the comparability of the surveys was assessed was based on an iterative process of reviewing the methods used by the four point prevalence surveys. This set of specifications focused on 3 fundamental elements of an indicator: the numerator, the denominator and items related to stratification. For each of these elements key items that point to comparability were described.
In the case of pressure ulcer definition, the classification presented in the international guideline co-published by the National Pressure Injury Advisory Panel, the European Pressure Ulcer Advisory Board and the Pan Pacific Pressure Injury Alliance is used for our study. Information on the definitions and methods used for each of the four point prevalence surveys was retrieved from published documents and information provided directly by the investigators involved in some of these point prevalence systems.
3、Results
3.1 Relevant key features of the four point prevalence measurement systems
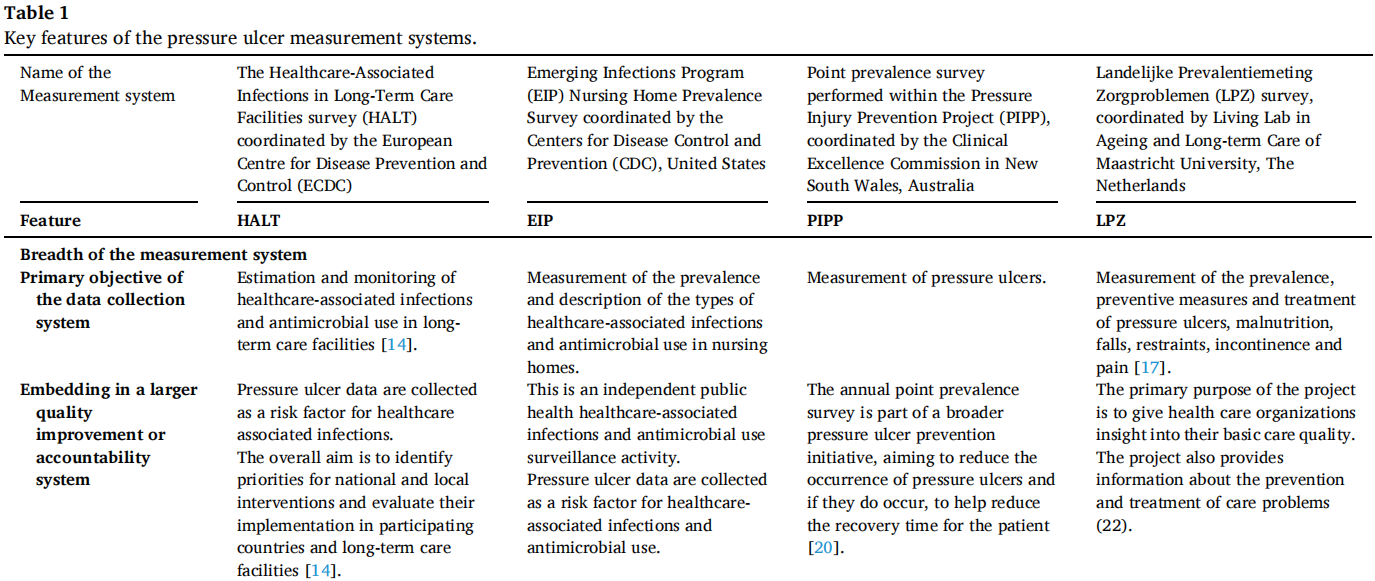
The key features of the point prevalence surveys are presented in Table 1. The breadth of the four surveys varies substantially. A major difference between the point prevalence systems is their purpose. The HALT and EIP surveys are focused on healthcare-associated infections and antimicrobial use, and pressure ulcer data are collected as a relevant risk factor. This is not the case for the PIPP and LPZ surveys, which put explicit emphasis on pressure ulcer data collection. All of the surveys are part of a broader quality improvement effort, where facility level data are intended for internal use by the surveyed facility and aggregated data are intended for the general public or policy-makers.
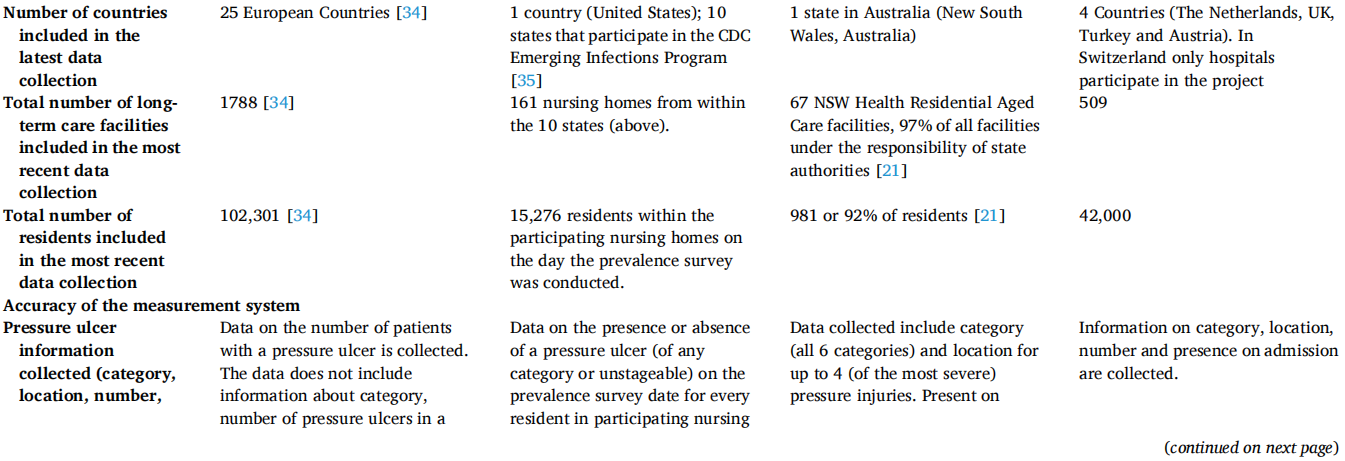

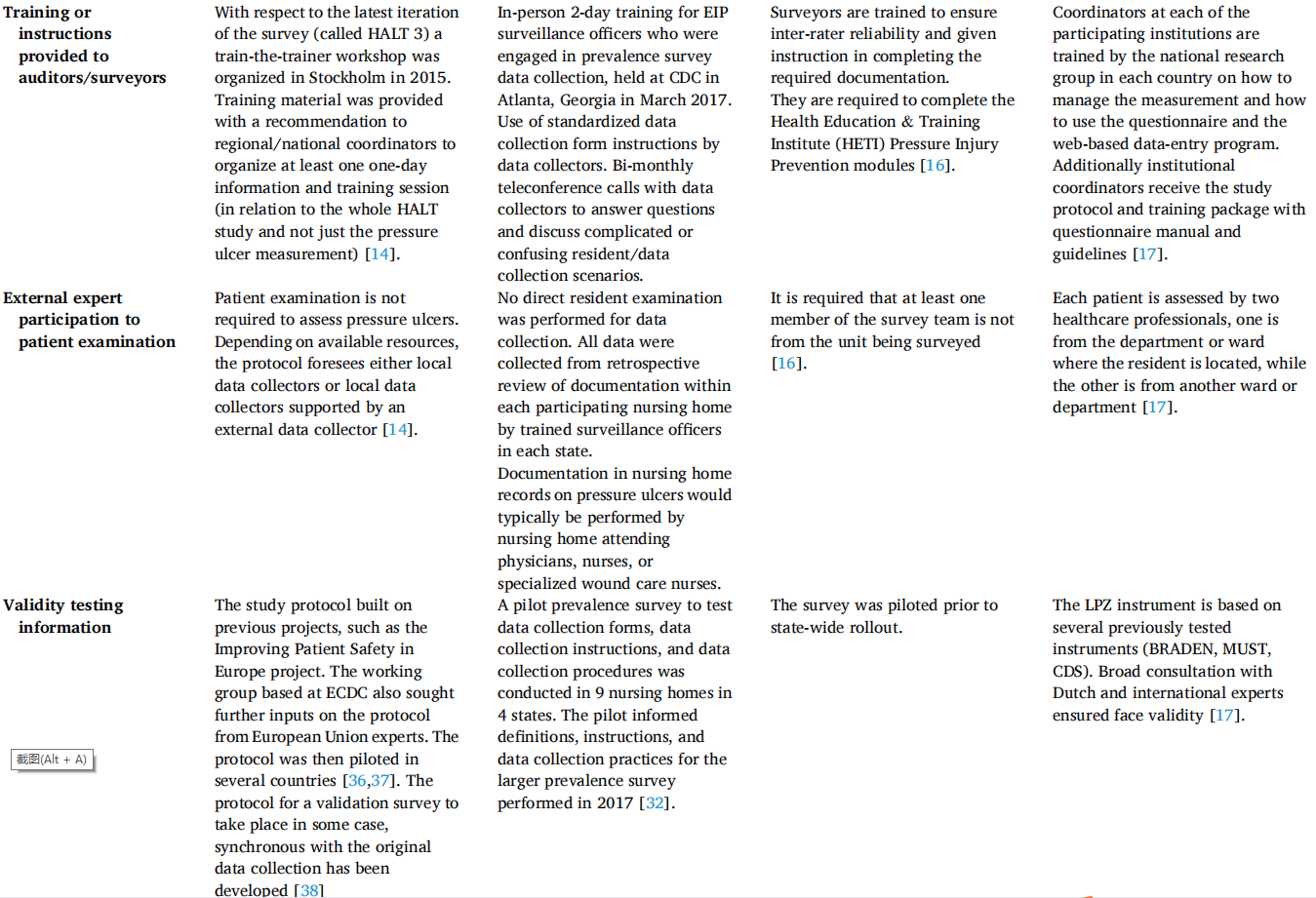

The PIPP and LPZ surveys, where pressure ulcer measurement is one of the principal aims, collected more detailed data on pressure ulcers, such as category (i.e., stage or grade) of the pressure ulcer or their location and presence on admission. Furthermore, these two measurement systems also require direct patient assessment for pressure ulcers by surveyors, while the HALT protocol does not explicitly require such an examination and the EIP survey is based on existing documentation in resident medical records. These findings suggest that the accuracy of the PIPP and LPZ surveys in measuring pressure ulcers is likely higher than the other two point prevalence systems. All four point prevalence surveys took action to train the surveyors and increase the validity and reliability of the surveys. However, the training and reliability and validity efforts were related to the survey methods and hence in the case of HALT and EIP were not focused on pressure ulcer measurement.
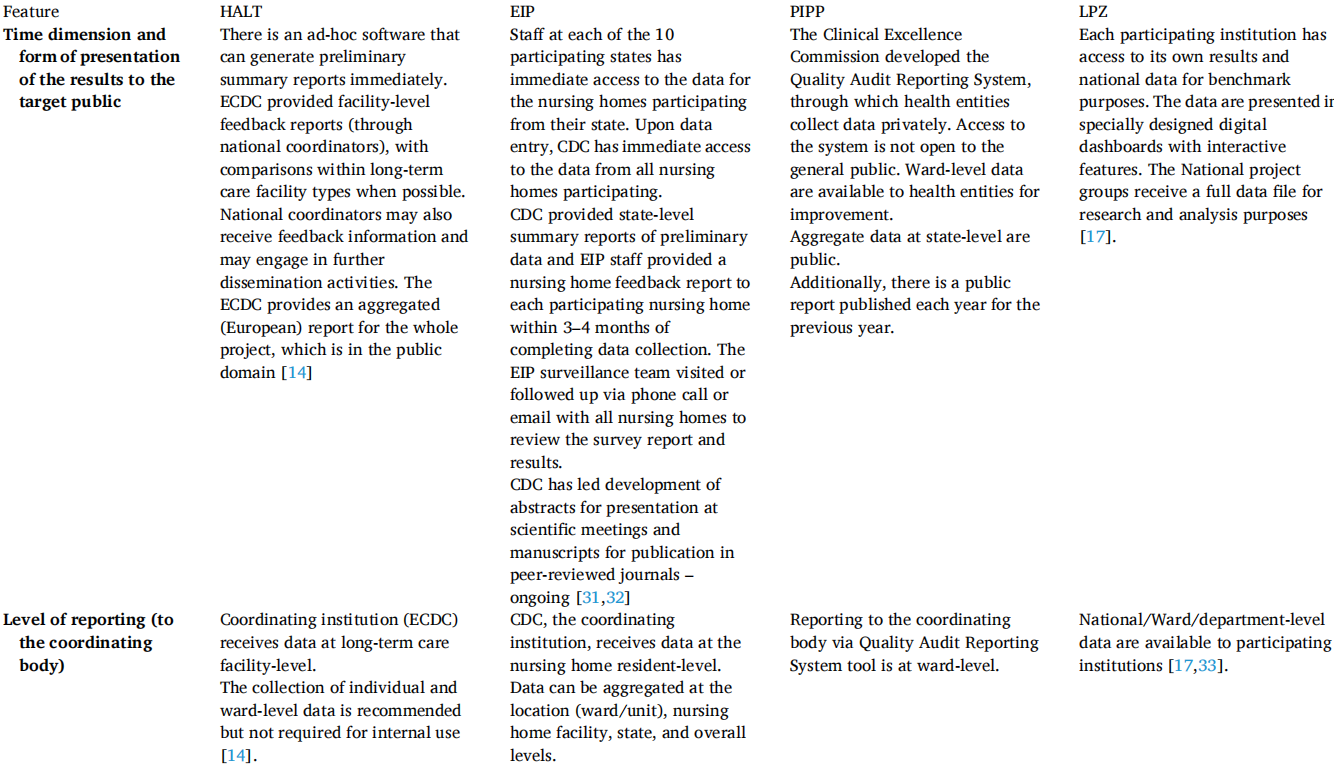
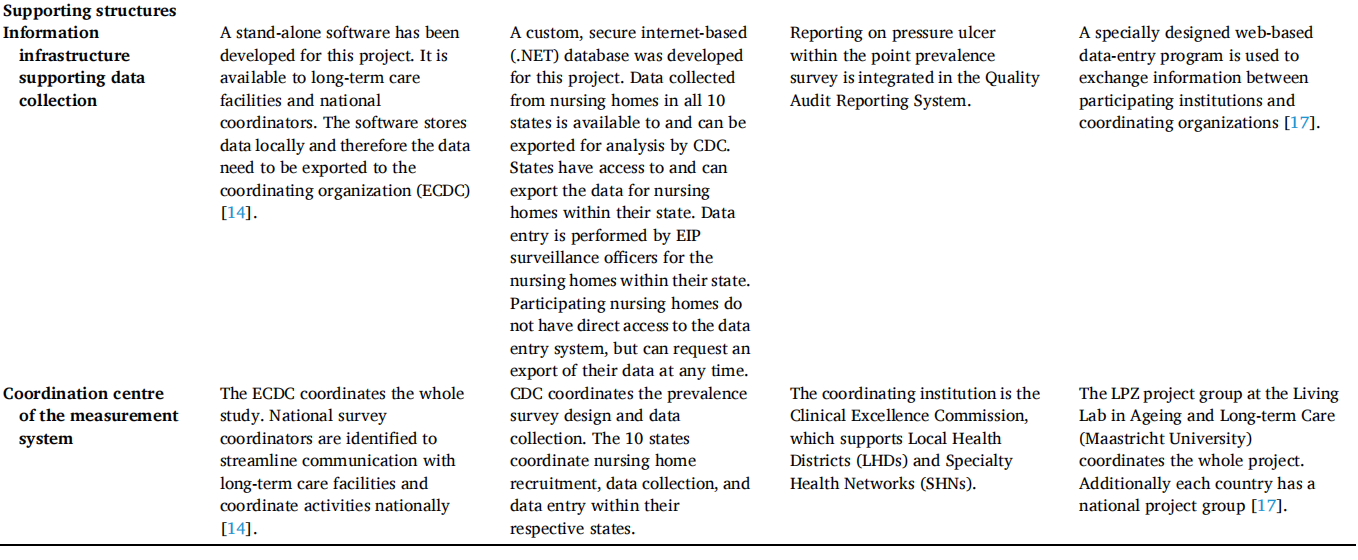
All four point prevalence systems use an ad hoc software or data collection interface. All of these four systems also have a two tier coordination arrangement, where in addition to the overall coordinating institution, there are local entities to streamline communication between long-term care facilities and the overall coordinating body. These local entities are national survey coordinators and national project groups in the case of HALT and LPZ, respectively, state public health authorities in the case of EIP, and so-called Local Health Districts and Specialty Health Networks in the case of PIPP.
3.2 Methodological comparability of the measurement systems
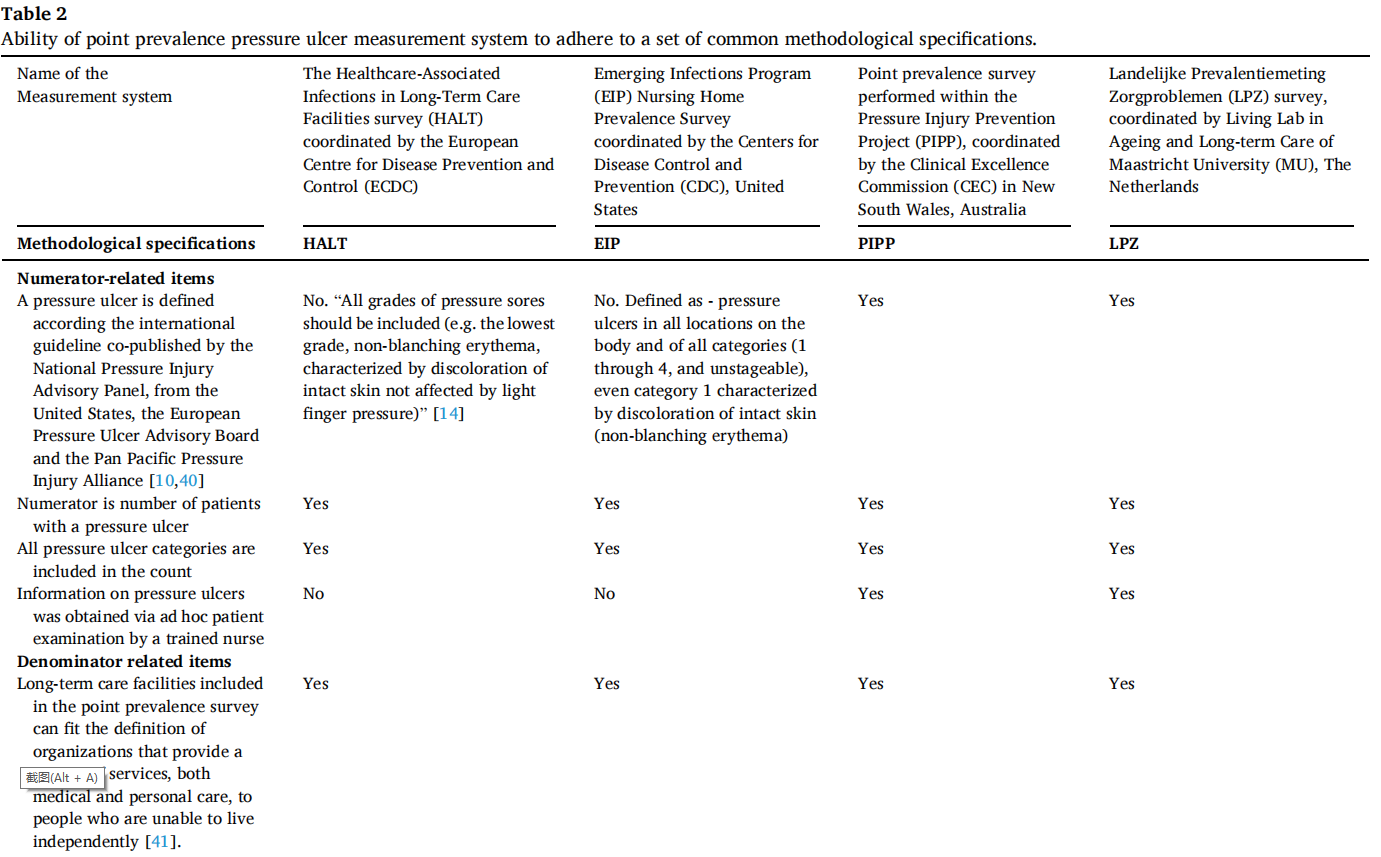
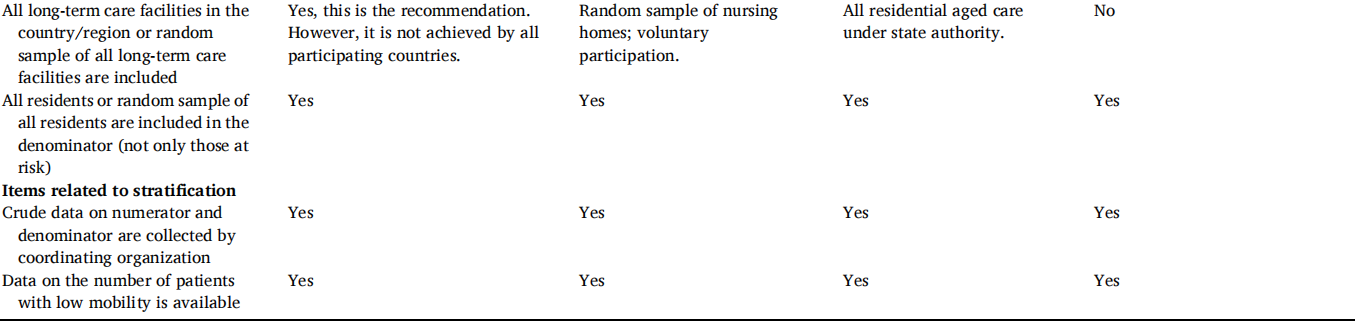
The ability of the four point prevalence measurement systems to adhere to common methodological specifications is presented in Table 2. Only the LPZ and PIPP point prevalence measurement systems make an explicit reference to the international guidelines [10,17,21]. The HALT protocol requires the inclusion of all pressure ulcer categories, however there is no explicit reference to deep tissue injury or unstageable pressure ulcers [14]. The CDC survey includes the four pressure ulcer categories and unstageable pressure ulcers, but no explicit reference is made to deep tissue injury. At the same time all of the four point prevalence systems gather data on the number of patients with pressure ulcers (as opposed to the total number of pressure ulcers, for example) and include category 1 pressure ulcers.
A common definition for long-term care facilities was formulated as reported in Table 2. Nonetheless, this does not imply that the long-term care facilities included by the various point prevalence measurement systems are the same. The HALT survey for example identified five types of long-term care facilities (General nursing homes, Residential homes, Specialized long-term care facilities, Mixed long-term care facilities and Other long-term care facilities) [14], all of which can fit the general definition used in this analysis. Within the sample of eligible long-term care facilities in each point prevalence measurement system, the LPZ survey does not include a random sample of facilities, as participation to the survey is voluntary. The PIPP survey includes all of the long-term care facilities under the state authority, but these represent only part of the long-term care facilities in the state, as most fall under the authority of the central Australian Government. The EIP survey is based on a random sample of long-term care facilities, but participation is voluntary. The HALT protocol does recommend a random choice of long-term care facilities in each country, but not all participating countries are able to satisfy this requirement. The HALT survey also set out criteria to assess national representativeness of the sample of long-term care facilities [14]. All four point prevalence measurement systems require that all residents within the selected long-term care facility, department or unit are assessed.
Crude data are provided to the coordinating organization within all four point prevalence measurement systems. All four systems also collect information on impaired mobility, although the way they define it differs slightly. For example the HALT and EIP surveys collect data on “residents who need a wheel chair or are bedridden on the PPS [Point prevalence survey] day” [14] while the LPZ systems collect data on mobility on a 5 point scale based on the Care Dependency Scale [17].
4、Discussion
The four point prevalence measurement systems differ considerably on a number of features. The ability to correctly identify and classify pressure ulcers requires a physical assessment of the resident. The international guideline [10] explicitly recommends a head-to-toe skin assessment. The PIPP and LPZ surveys do require a skin assessment of the resident. In the case of the EIP survey this is not performed by surveillance officers collecting the prevalence survey data. However, the surveillance officers have access to nursing home documentation that has been shown to be highly reliable in pressure ulcer identification [42]. The HALT survey requires a review of the residents with health personnel, but not necessarily a skin assessment of the patient.
The ability to accurately distinguish patients who have a pressure ulcer from those who do not have one also relies on the case definition of pressure ulcer and the classification related to it [30,43]. Despite the availability of an international guideline on pressure ulcer definition and classifications [10], two of the four measurement systems analyzed do not make an explicit reference to it. Their definitions of what is considered a pressure ulcer do not contradict the international guideline definition, but also do not clarify whether suspected deep tissue injury should be included in the count or not.
The lack of explicit guidelines on deep tissue injury in the HALT and EIP surveys and on unstageable pressure ulcer in the HALT survey may hamper comparability [9,28]. However, it should be noted that these types of pressure ulcers are not very common. On the contrary, category 1 pressure ulcers are the most frequent category present [44,45]. In the latest report of the PIPP survey [21], 64% of all pressure ulcers acquired in the long-term care facility were classified as category 1. A recent systematic review of pressure ulcers in Europe calculated a mean percentage of category 1 pressure ulcer to be 32.35% [46]. Errors in classifying category 1 pressure ulcer may therefore lead to important differences in pressure ulcer prevalence counts. The correct identification of category 1 pressure ulcer was relatively low in several studies [47,48].
The accuracy of pressure ulcer monitoring may be increased by excluding category 1 pressure ulcer from the count. Category 1 pressure ulcer are indeed not included in several pressure ulcer reports [28,33, 49]. As practices in excluding category 1 pressure ulcer tend to differ between studies [50,51], both the HALT and the EIP surveys explicitly mentioned that category 1 pressure ulcer (non-blanchable erythema) is to be included in the data collection. It is worth noting that category 1 pressure ulcers are clinically important, despite challenges in accurate measurement [52,53]. If data on pressure ulcer category were collected by all point prevalence measurement systems, it would also be possible to compare data on pressure ulcer prevalence excluding category 1. This might provide an additional piece of information about the comparability of the measurement systems, without loss of important clinical information.
Another crucial aspect for accurate monitoring of pressure ulcers is the ability to correctly identify pressure ulcers. Kottner et al. [43] in their systematic review found high interrater reliabilities of pressure ulcer classification based on skin examination. However, they also found that the studies considered included raters “specialized, trained or experienced in pressure ulcer diagnosis” [43]. On the other hand, when a convenience sample of nurses from five European countries was surveyed, the reliability of their classification of pressure ulcer based on photographs was considerably lower [47]. Training can improve the ability of nurses to correctly identify pressure ulcers [54]. The training reported in the results section above refers to the overall point prevalence measurement systems and is not necessarily limited to training in pressure ulcer identification and classification. In particular the HALT survey may not emphasize the training in pressure ulcer identification and classification, as pressure ulcers are not the main focus of the survey. The same also holds for the EIP survey, but in that case surveillance officers were reliant on the documentation in resident medical records to identify pressure ulcers.
The denominator in all four measurement systems is represented by all residents of the unit of the long-term care facility being surveyed on the day of the survey. However, the long-term care facilities included in the denominator do not necessarily serve residents with similar needs and health status. Several studies have found varying proportions of the older population residing in long-term care facilities and different residents characteristics in different countries [55,56]. These differences are also apparent when the number of long-term care beds relative to the size of the population aged 65 and over in different countries is compared [3]. A concern may arise when comparing long-term care facilities with different purposes or characteristics that potential differences in the susceptibility of the residents (i.e. the population in the denominator) to develop pressure ulcers might limit comparability. Considering the heterogeneity of long-term care facilities described above, the best approach to take into account these differences is to include information on risk factors for pressure ulcer development.
There are several risk factors for pressure ulcer development [10]. Those that emerge most frequently as independent risk factors have been grouped by Coleman et al. [57] in three domains: mobility/activity, perfusion (including diabetes) and skin/pressure ulcer status. While all four point prevalence measurement systems analyzed collect data on mobility, the way that mobility was defined differs; all four can identify residents with severe mobility limitations for the purpose of comparability. Several tools exist to assess the risk of developing a pressure ulcer [58,59] which, if integrated into the measurement systems, could be used to provide a measure for the susceptibility of residents to develop pressure ulcers. These tools, however, require additional data which are not currently collected by all of the four point prevalence measurement systems under consideration.
It is important to note that the HALT survey protocol includes recommendations, such as the minimum number of long-term care facilities per country, to which countries adhere to a varying extent, as difference in representativeness and deviations from recommended country sample sizes indicate [14,34]. While this premise weakens the comparability of the findings, it might also be necessary, to allow enough flexibility for each country to implement the protocol to the extent that the resources and engagement of each country on the issue allow.
A few low resource interventions might improve the quality of the pressure ulcer measurement in particular in the case of the HALT and EIP surveys, which are not focused on pressure ulcers, such as clarifying the definition of pressure ulcer and collecting data on the category of pressure ulcer identified. The quality of the collected data may be increased by ensuring that a resident head-to-toe assessment is the basis of pressure ulcer data collection. This would also imply the need for the point prevalence measurement system training to include pressure ulcer recognition and classification. However, such an intervention is resource intensive, may have legal, ethical and other implications in some countries. Alternatively, assurances may be sought of the reliability of existing pressure ulcer data that surveyors could use.
It is also important to consider the intended use of the performance measures. Small variations in quality of data collection may not be acceptable for a nursing home fine-tuning its pressure ulcer prevention activities, but might be acceptable for country comparisons, where the purpose of such comparison is for countries to recognize whether they are outliers on pressure ulcer prevalence with respect to their peers. Such outliers may find that they need to pay more attention to the issue of pressure ulcer in long-term care facilities nationwide. A recent publication of the OECD based on pressure ulcer data from the HALT and EIP surveys showed a 14-fold difference in prevalence rates between the best and worst performers [3]. Caution is necessary in interpreting these differences. The precision of prevalence rates is impacted by factors such as the number of participating institutions and included residents. Our analysis suggests that other factors, such as representativeness of the sample and approach to data collection, are also important.
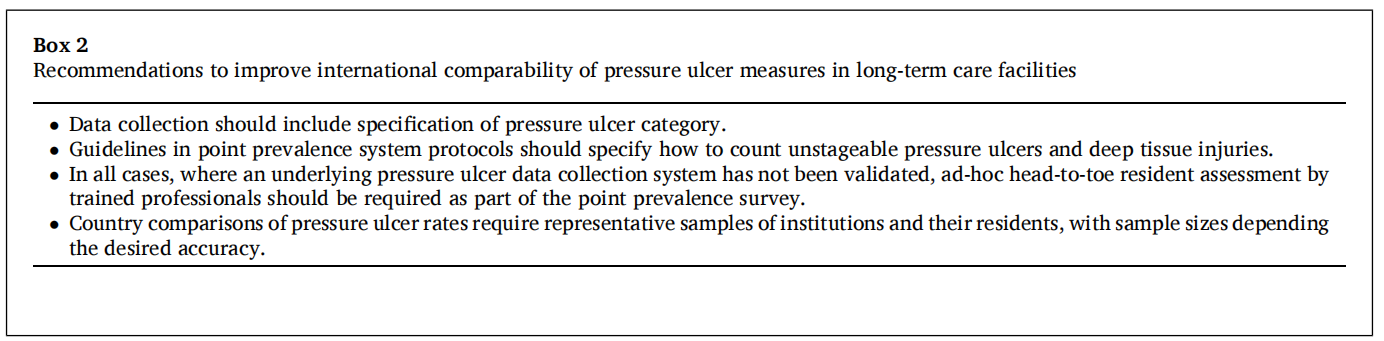
The LPZ and the PIPP surveys use relatively resource intensive pressure ulcer measurement methods, which provide data of good quality but present the challenge of scalability. The PIPP survey is limited to a group of long-term care facilities in one Australian state. The LPZ survey, which has an international breadth, involves voluntary participation of long-term care facilities. The latter can be assumed to have a high level of commitment to the issue of pressure ulcer, which limits country representativeness of the findings. The HALT and EIP surveys have some limitations in the quality of the measurement systems as explained above, which are likely related to the fact that the point prevalence measurement systems are not focused on pressure ulcer measurement. If the pressure ulcer identification accuracy and sample representativeness limitations could be overcome, the pressure ulcer values provided by the four point prevalence measurement systems would be comparable for the purpose of steering policies at national level. All recommendations to improve international comparability of pressure ulcer rates are summarized in Box 2.
4.1 Strength and limitations
Our analysis includes point prevalence measurement systems used in 28 high- and middle-income countries on three continents, thus providing a strong international perspective.
We focused specifically on four point prevalence measurement systems; additional observations might be drawn from analyzing other point prevalence measurement systems aimed at monitoring pressure ulcers. There are also other measures of pressure ulcers, in particular incidence measures, which can be derived from long-term care facilitybased surveillance systems. A separate but equally important line of investigation would be to assess the quality, international comparability and availability of measures obtained from such data collection systems.
5、Conclusions
The four point prevalence measurement systems analyzed vary in some of their key features. They use different classifications of pressure ulcers and different approaches to data collection. The methods to select and include long-term care facilities by country also differs among the measurement systems.
In principle it is possible to harmonize the approaches of these measurement systems. The comparability of the pressure ulcer count depends partly on using a compatible pressure ulcer classification system and either a head-to-toe skin assessment, supported by ad hoc training or validated pre-existing documentation. If inferences are to be made about pressure ulcer prevalence in long-term care facilities by country, then the country representativeness of a comparable long-term care facility sample is another crucial element. Some of the adaptations necessary to increase comparability can be implemented through minor changes in the survey protocols. Other adaptations are more resource intensive and may be less feasible in certain countries. Coordinating bodies of these point prevalence measurement systems should consider the risk and benefits of adapting their systems to enhance international comparability of pressure ulcers measures in long-term care facilities. The comparability of the measures will support learning across countries with the aim to facilitate improvements in pressure ulcer prevention and treatment and ultimately result in increased resident safety.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
1、Oecd. European union. A good life in old age? Paris: OECD Publishing; 2013.
2、Edvardsson D, Baxter R, Corneliusson L, Anderson RA, Beeber A, Boas PV, et al.Advancing long-term care science through using common data elements: candidate measures for care outcomes of personhood, well-being, and quality of life. Gerontology & geriatric medicine 2019;5. 2333721419842672.
3、Oecd. Health at a glance 2019. Paris: OECD Publishing; 2019.
4、Frijters DH, van der Roest HG, Carpenter IG, Finne-Soveri H, Henrard JC, Chetrit A, et al. The calculation of quality indicators for long term care facilities in 8 countries (SHELTER project). BMC Health Serv Res 2013;13:138.
5、Tolson D, Rolland Y, Katz PR, Woo J, Morley JE, Vellas B. An international survey of nursing homes. J Am Med Dir Assoc 2013;14(7):459–62.
6、Adair CE, Simpson E, Casebeer AL, Birdsell JM, Hayden KA, Lewis S. Performance measurement in healthcare: part II–state of the science findings by stage of the performance measurement process. Healthcare policy = Politiques de sante 2006;2 (1):56–78.
7、Beaussier AL, Demeritt D, Griffiths A, Rothstein H. Steering by their own lights:why regulators across Europe use different indicators to measure healthcare quality. Health Pol 2020;124(5):501–10.
8、Heslop L, Lu S. Nursing-sensitive indicators: a concept analysis. J Adv Nurs 2014;70(11):2469–82.
9、Pieper B. Pressure ulcers: prevalence, incidence, and implications for the future.Washington, D.C.: National Pressure Ulcer Advisory Panel; 2012.
10、European pressure ulcer advisory Panel, national pressure injury advisory Panel, Pan pacific pressure injury alliance. Prevention and treatment of pressure ulcers/injuries: clinical practice guideline. The international guideline. EPUAP/NPIAP/PPPIA; 2019.
11、Strengthening OECD. Health information infrastructure for health care quality governance. Paris: OECD Publishing; 2013.
12、Mor V, Finne-Soveri H, Hirdes JP, Gilgen R, Dupasquier J-N. Long-term care quality monitoring using the inteRAI common clinical assessment language.Performance Measurement for Health System Improvement: experiences,Challenges and Prospects. Cambridge: Cambridge University Press; 2010.
13、Spasova S, Baeten R, Coster S, Ghailani D, Pena-Casas R, Vanhercke B. Challenges in long-term care in Europe. A study of national policies. Brussels: European Commission; 2018.
14、European Centre for Disease Prevention and Control. Protocol for point prevalence surveys of healthcare-associated infections and antimicrobial use in European long term care facilities - version 2.1. Stockholm: ECDC; 2016.
15、Thompson ND, Brown CJ, Eure T, Penna A, Bamberg W, Barney G, et al. 1831. Point prevalence and epidemiology of antimicrobial use in US nursing homes, 2017. Open Forum Infect Dis 2018;5(Suppl 1):S521–.
16、Clinical Excellence Commission. 2016 NSW pressure injury point prevalence survey guide. Sydney: Clinical Excellence Commission; 2016.
17、van Nie-Visser NC, Schols JM, Meesterberends E, Lohrmann C, Meijers JM,Halfens RJ. An international prevalence measurement of care problems: study protocol. J Adv Nurs 2013;69(9):e18–29.
18、European Centre for Disease Prevention and Control. About the point prevalence survey of healthcare-associated infections and antimicrobial use in European long term care facilities. https://www.ecdc.europa.eu/en/infectious-diseases-public-he alth/healthcare-associated-infections-long-term-care-facilities-1.
19、Centers for Disease Control and Prevention. About EIP 2018. https://www.cdc. gov/ncezid/dpei/eip/eip-about.html.
20、Clinical Excellence Commission. Pressure injury prevention. http://www.cec.health.nsw.gov.au/keep-patients-safe/pressure-injury.
21、Clinical Excellence Commission. 2018 NSW Prssure injury point prevalence survey report. Sydney: Clinical Excellence Commission; 2019.
22、Maastricht University Caphri Departmen of Health. Abouth the LPZ. https://nl.lpzum.eu/nl/Home/About.
23、Institute of Medicine Committee on the National Quality Report on Health Care Delivery. Envisioning the national health care quality report. Washington, D.C.: National Academies Press; 2001.
24、Barbazza E, Klazinga NS, Kringos D. Exploring the actionability of health care performance indicators on quality of care: what makes an indicator fit for purpose and use? under review. 2020.
25、Forde I, Morgan D, Klazinga NS. Resolving the challenges in the international comparison of health systems: the must do’s and the trade-offs. Health Pol 2013; 112(1):4–8.
26、Requejo JH, Newby H, Bryce J. Measuring coverage in MNCH: challenges and opportunities in the selection of coverage indicators for global monitoring. PLoS Med 2013;10(5):e1001416.
27、Gunningberg L, Donaldson N, Aydin C, Idvall E. Exploring variation in pressure ulcer prevalence in Sweden and the USA: benchmarking in action. J Eval Clin Pract 2012;18(4):904–10.
28、Smith IL, Nixon J, Brown S, Wilson L, Coleman S. Pressure ulcer and wounds reporting in NHS hospitals in England part 1: audit of monitoring systems. J Tissue Viability 2016;25(1):3–15.
29、Coleman S, Smith IL, Nixon J, Wilson L, Brown S. Pressure ulcer and wounds reporting in NHS hospitals in England part 2: survey of monitoring systems. J Tissue Viability 2016;25(1):16–25.
30、Vanderwee K, Clark M, Dealey C, Gunningberg L, Defloor T. Pressure ulcer prevalence in Europe: a pilot study. J Eval Clin Pract 2007;13(2):227–35.
31、Thompson ND, Penna A, Eure TR, Bamberg WM, Barney G, Barter D, et al. Epidemiology of antibiotic use for urinary tract infection in nursing home residents. J Am Med Dir Assoc 2020;21(1):91–6.
32、Epstein L, Stone ND, LaPlace L, Harper J, Lynfield R, Warnke L, et al. Comparison of data collection for healthcare-associated infection surveillance in nursing homes. Infection control and hospital epidemiology 2016;37(12):1440–5.
33、Halfens RJ, Meesterberends E, van Nie-Visser NC, Lohrmann C, Schonherr S, Meijers JM, et al. International prevalence measurement of care problems: results. J Adv Nurs 2013;69(9):e5–17.
34、Ricchizzi E, Latour K, K¨arkiT, Buttazzi R, Jans B, Moro ML, et al. Antimicrobial use in European long-term care facilities: results from the third point prevalence survey of healthcare-associated infections and antimicrobial use, 2016 to 2017. Euro Surveill 2018;23(46).
35、Centers for Disease Control and Prevention. HAI and antibiotic use prevalence survey https://www.cdc.gov/hai/eip/antibiotic-use.html.
36、European Centre for Disease Prevention and Control. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals. Stockholm: ECDC; 2013.
37、Hansen S, Sohr D, Geffers C, Astagneau P, Blacky A, Koller W, et al. Concordance between European and US case definitions of healthcare-associated infections. Antimicrob Resist Infect Contr 2012;1(1):28.
38、European Centre for Disease Prevention and Control. Protocol for validation of point prevalence surveys of healthcare-associated infections and antimicrobal use in European long-term care facilities - 2016-2017 version 1.1. Stockholm: ECDC;2016.
39、Clinical Excellence Commission. Clinical excellence pressure injury prevention project monitoring & auditing framework. Syndey: Clinical Excellence Commission; 2014.
40、Panel NPUA, Panel EPUA, Alliance PPPI. In: Heasler E, editor. Prevention and treatment of pressure ulcers: clinical practice guidelines. Osborne Park, Western Australia: Cambridge Media; 2014.
41、Center for Disease Control and Prevention. Nursing homes and assisted living (Long-term care facilities [LTCFs]). https://www.cdc.gov/longtermcare/index.html.
42、Mor V, Angelelli J, Jones R, Roy J, Moore T, Morris J. Inter-rater reliability of nursing home quality indicators in the U.S. BMC Health Serv Res 2003;3(1):20.
43、Kottner J, Raeder K, Halfens R, Dassen T. A systematic review of interrater reliability of pressure ulcer classification systems. J Clin Nurs 2009;18(3):315–36.
44、Gunningberg L, Hommel A, Baath C, Idvall E. The first national pressure ulcer prevalence survey in county council and municipality settings in Sweden. J Eval Clin Pract 2013;19(5):862–7.
45、Tannen A, Bours G, Halfens R, Dassen T. A comparison of pressure ulcer prevalence rates in nursing homes in The Netherlands and Germany, adjusted for population characteristics. Res Nurs Health 2006;29(6):588–96.
46、Moore Z, Avsar P, Conaty L, Moore DH, Patton D, O’Connor T. The prevalence of pressure ulcers in Europe, what does the European data tell us: a systematic review. J Wound Care 2019;28(11):710–9.
47、Beeckman D, Schoonhoven L, Fletcher J, Furtado K, Gunningberg L, Heyman H,et al. EPUAP classification system for pressure ulcers: European reliability study. J Adv Nurs 2007;60(6):682–91.
48、Defloor T, Schoonhoven L, Katrien V, Weststrate J, Myny D. Reliability of the European pressure ulcer advisory Panel classification system. J Adv Nurs 2006;54 (2):189–98.
49、Ahn H, Cowan L, Garvan C, Lyon D, Stechmiller J. Risk factors for pressure ulcers including suspected deep tissue injury in nursing home facility residents: analysis of national minimum data set 3.0. Adv Skin Wound Care 2016;29(4):178–90. quiz E1.
50、Moore Z, Johanssen E, van Etten M. A review of PU prevalence and incidence across Scandinavia, Iceland and Ireland (Part I). J Wound Care 2013;22:4–8. 7): 361-2.
51、Anthony D, Alosoumi D, Safari R. Prevalence of pressure ulcers in long-term care: a global review. J Wound Care 2019;28(11):702–9.
52、Shi C, Bonnett LJ, Dumville JC, Cullum N. Nonblanchable erythema for predicting pressure ulcer development: a systematic review with an individual participant data meta-analysis. Br J Dermatol 2020;182(2):278–86.
53、Kottner J. The clinical relevance of nonblanchable erythema in pressure ulcer prevention. Br J Dermatol 2020;182(2):262–3.
54、Park M, Kim G, Kim K. The effect of pressure injury training for nurses: a systematic review and meta-analysis. Adv Skin Wound Care 2020;33(3):1–11.
55、Onder G, Carpenter I, Finne-Soveri H, Gindin J, Frijters D, Henrard JC, et al.Assessment of nursing home residents in Europe: the services and health for elderly in long TERm care (SHELTER) study. BMC Health Serv Res 2012;12:5.
56、Ribbe MW, Ljunggren G, Steel K, Topinkov´aE, Hawes C, Ikegami N, et al. Nursing homes in 10 nations: a comparison between countries and settings. Age Ageing 1997;26(Suppl 2):3–12.
57、Coleman S, Gorecki C, Nelson EA, Closs SJ, Defloor T, Halfens R, et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud 2013;50 (7):974–1003.
58、Moore ZEH, Patton D. Risk assessment tools for the prevention of pressure ulcers.Cochrane Database Syst Rev 2019;(1).
59、Park SH, Lee YS, Kwon YM. Predictive validity of pressure ulcer risk assessment tools for elderly: a meta-analysis. West J Nurs Res 2016;38(4):459–83.
Acknowledgements
The authors would like to thank Irma Everink from the Living Lab in Ageing and Long-term Care of Maastricht University and Maree Connolly from the Clinical Excellence Commission in New South Wales for the information about pressure ulcer measurement systems they provided. The authors would also like to thank the staff from CDCs Emerging Infections Program (EIP) who participated in the Nursing Home Prevalence Survey.

