Introduction
Split-thickness skin graft (STSG) remains the most frequently used reconstructive option for skin and soft tissue defects1,2. The procedure involves harvesting of the full epidermis and part of the dermis, but creates a secondary wound at the donor site. Patients may experience donor-site discomfort (pain and itching), delayed healing and infection, an unsatisfactory cosmetic appearance and reduced quality of life3–6. Co-morbidities such as ageing, poor nutrition, immobility, smoking, diabetes and peripheral vascular disease contribute to impaired donor-site henaling.
Current therapeutic strategies for STSG donor sites are focused on creating an optimal environment that allows rapid re-epithelialization by accelerating keratinocyte proliferation and angiogenesis, while preventing infection, minimizing patient discomfort and promoting a good cosmetic outcome3–6. A wide variety of novel wound dressings have been proposed for donor-site management. There is evidence that hydrocolloid dressings facilitate fastest healing and minimal patient discomfort5–9. However, despite optimal conditions, donor-site re-epithelialization may typically take 7–21 days5,6,8.
Cell-based therapeutic strategies including use of stem cells10 –12 and autologous skin cells13,14 are increasingly important for the treatment of open wounds, and may improve tissue repair and accelerate skin regeneration. Autologous, non-cultured, heterogeneous skin cell suspension, which can be obtained using the ReCell® system (Avita Medical, Cambridge, UK), includes 65 percent keratinocytes, 30 per cent fibroblasts and 3⋅5 percent melanocytes15. With only a small donor population of autologous basal layer cells, patients can be treated immediately without the need for culture and expansion of the cell suspension. In the disaggregated state, these viable skin cells are free from contact inhibition, and are capable of adhering to a wound surface and proliferating to accelerate wound repair and re-epithelialization in burn wounds and chronic ulcers16–19. Moreover, as the cell suspension contains viable melanocytes, it has been used on pigmentation lesions such as in vitiligo and congenital melanocytic naevus to improve repigmentation20,21. Hu and colleagues22 recently reported in a randomized trial that the autologous skin cell suspension combined with a split-thickness skin autograft improved chronic wound healing and long-term aesthetic appearance22. Similarly, Campanella and co-workers23 reported comparative results of a silicone dressing and a monofilament polyamide woven dressing on paediatric donor sites treated with skin cells obtained by the ReCell® system.
The present study was conducted to investigate whether autologous skin cell suspension treatment could promote donor-site wound healing, reduce morbidities such as pain and itching, and achieve better aesthetic outcomes. An RCT was conducted to compare standard care (non-occlusive hydrocolloid dressing; Urgotul®, Laboratories Urgo, Chenôve, France)6,24, with and without autologous skin cell treatment.
Methods
A randomized single-blind clinical trial (subjects blinded to treatment) was conducted from September 2014 to February 2016 in the First Affiliated Hospital of Sun Yat-sen University. This trial was approved by hospital institutional review board. Consecutive patients requiring STSG were enrolled in the trial; all subjects provided written informed consent.
Eligible patients were men or non-pregnant women,between 18 and 80 years of age, who had a single donor site after STSG harvesting for any indication with a surface area larger than 20 cm2. In patients with multiple donor sites, the allocated treatment was used on all wounds, but only the largest donor site meeting the inclusion criteria was chosen as the target to study. Exclusion criteria comprised: pre-existing medical conditions that could potentially interfere with wound healing (malignancy, autoimmune disease, chemotherapy, corticosteroid use, skin disease or local irradiation), renal failure (glomerular filtration rate below 60 ml/min) and refusal to give consent. Patients were enrolled by clinical physicians or a study nurse after diagnosis.
Patients were assigned randomly in a 1 : 1 ratio to two groups after informed consent. A computer-generated random allocation sequence with six-block size, designed by a third-party statistician, was used to assign subjects to the allocated treatment; this was provided to the investigator team in sequentially numbered, sealed envelopes on the day before surgery. The experimental group received autologous cell suspension and hydrocolloid dressing (Urgotul®) whereas the control group received only the hydrocolloid dressing (Urgotul®).
Surgical procedure
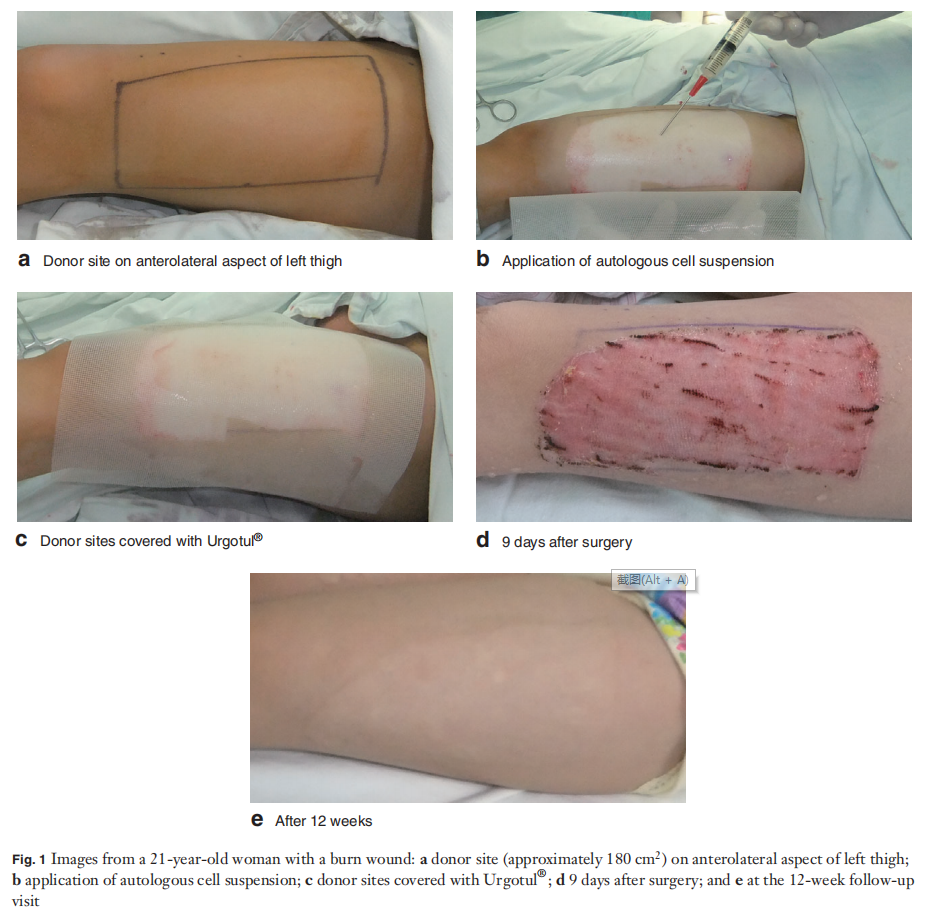
All operations were performed by the same surgeon. Under general anaesthesia, a STSG (thickness 0⋅25 mm) was harvested from the anterolateral aspect of the thigh using a Zimmer® dermatome (Zimmer, Dover, Ohio, USA). In the experimental group, a portion of skin from the STSG was processed using the ReCell® kit according to the manufacturer’s instructions, and reapplied to the donor sites in the form of skin cell suspension (Fig. 1). A biopsy area of 1 cm2 was required to treat a donor site of 80 cm2, to achieve a cellular spread rate of 1 : 8022. Treated donor sites were covered with the non-adherent hydrocolloid dressing (Urgotul®) and then wrapped with conventional gauze dressing.
Patients in the control group received Urgotul® alone over the donor site without application of the autologous skin cell suspension, Thereafter, care procedures were identical in both groups.
Postoperative care and follow-up
Donor-site dressings were changed by an experienced nurse on postoperative day 3 and repeated every second day until complete wound re-epithelialization. At each follow-up visit, Urgotul® was used as the primary dressing and followed by conventional bandages. When a donor-site infection was suspected, povidone–iodine ointment (QingFa Pharmaceutical, Guangdong, China) was added to a fresh primary dressing. Additional cleansing or protection during dressing changes was allowed in both groups. Patients were followed up for 12 weeks after complete wound re-epithelialization. After STSG harvest and during each follow-up visit, serial donor-site photographs were taken with a digital camera to evaluate the physical appearance of donor sites and quality of healing.
Outcomes
Treatment outcomes were evaluated until either complete wound closure or postoperative day 28. The primary endpoint was time to complete re-epithelialization, defined as covering of all affected areas without any persisting scabs. Complete wound healing was assessed by an experienced blinded plastic surgeon. Serial wound photographs were also reviewed by an expert in wound care who was blinded to treatment group assignment. Both independent reviewers assessed the time to complete donor-site healing, and obtained the same time to complete donor-site re-epithelialization, in all but two patients. Disagreements were resolved by discussion to reach a consensus. The interclass correlation coefficient was 0⋅997 for the time to re-epithelialization, indicating near complete reliability.
Secondary endpoints, included pain and itching, were measured on a standard visual analogue scale, ranging from 0 (none) to 10 (maximum)5,23. Treatment-related complications such as infection, haematoma, allergic reaction and overgranulation were assessed. The quality of donor sites was evaluated by means of the Patient and Observer Scar Assessment Scale (POSAS), which uses a range of scores from 6 (best) to 60 (worst), after complete healing of the donor site for 12 weeks5,23,25.
Statistical analysis
Sample size calculation was based on the primary outcome – time to complete re-epithelialization. To detect 20 per cent quicker wound healing with a 5 per cent significance level and a power of 80 per cent, a sample size of 53 patients per group was found to be necessary (at least 106 participants in total), given an anticipated dropout rate of 10 per cent.
Data were analysed using SPSS® for Windows® version 16.0 (IBM, Armonk, New York, USA) based on an intention-to-treat (ITT) group that included all randomly assigned patients. Continuous data are presented as mean(s.d.), and POSAS, pain and itching scores as median (i.q.r.), with analysis by Student’st test and Mann–Whitney U test respectively. χ2 test or Fisher’s exact test was used to compare categorical variables. Kaplan–Meier survivorship analysis was used to assess donor-site wound healing by time to complete re-epithelialization, and the log rank test to identify significant differences between survival curves. P <0⋅050 was considered indicative of statistical significance.
Results
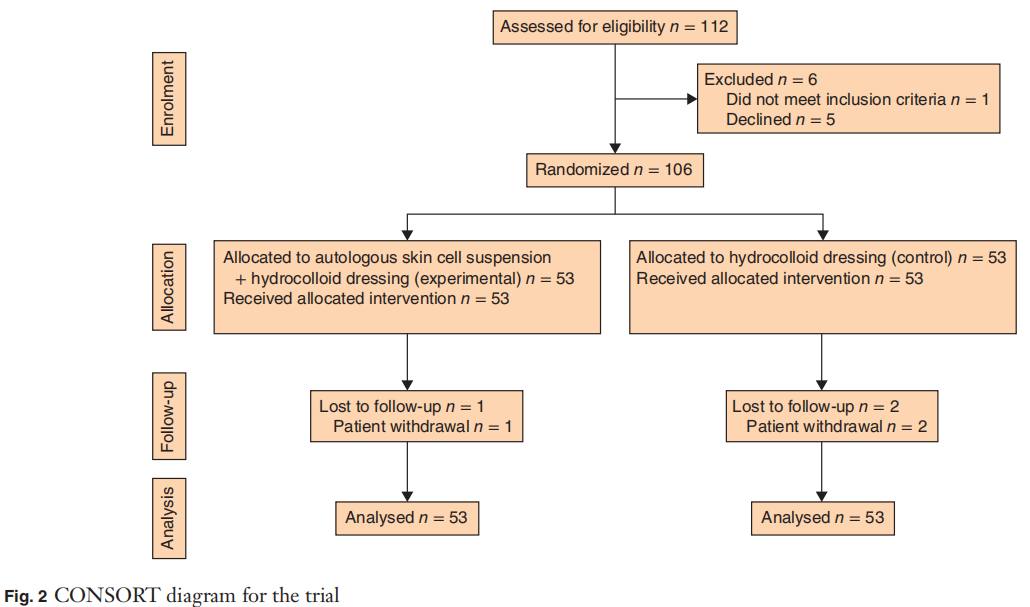
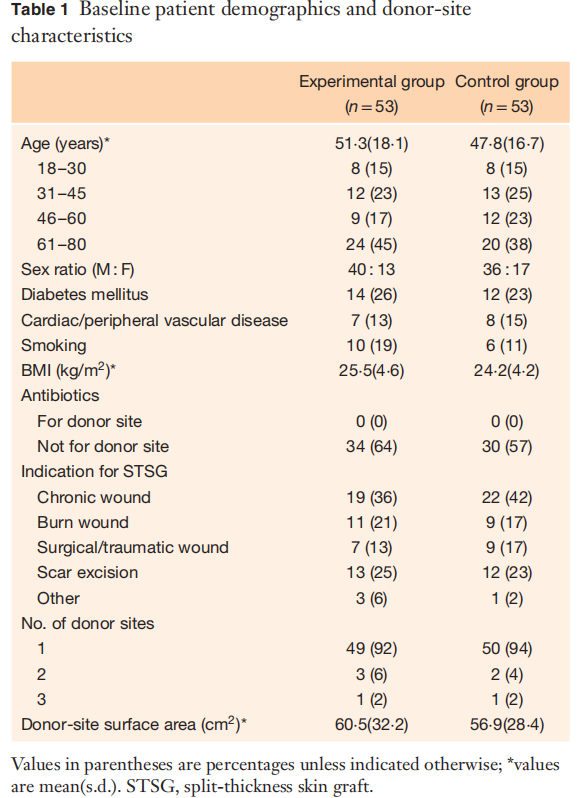
From September 2014 to February 2016, 112 patients were screened for inclusion, of whom six were excluded based on inclusion/exclusion criteria (1 patient), or declined to participate (5 patients). Thus, 106 patients were randomized to the experimental group (53 patients) or the control group (53). Of these, three patients did not complete follow-up after discharge from the hospital but were included in the ITT analysis (Fig. 2). The groups had similar patient demographics, co-morbidities and donor-site wound characteristics (Table 1). The mean(s.d.) age of the patients was 49⋅6(17⋅4) years, and most were men (71⋅7 percent). Forty-nine patients (92 per cent) in the experimental group and 50 (94 per cent) in the control group had one split-thickness donor site. The mean size of the donor-site wound was 58⋅7(30⋅3) cm2.
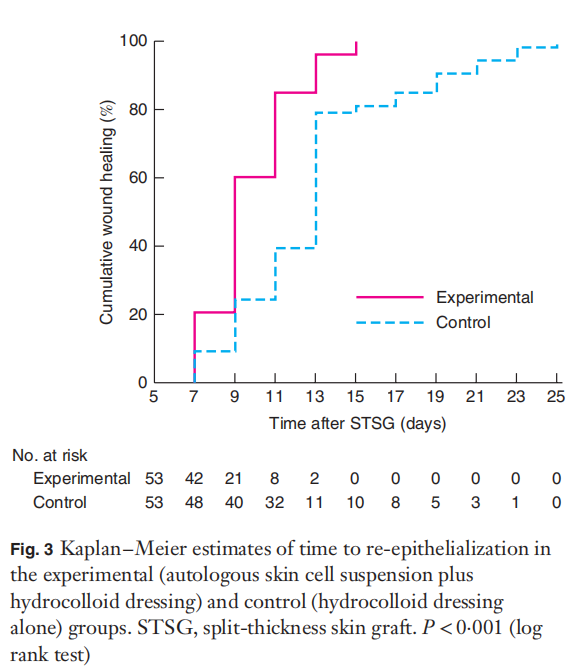
Donor sites in the experimental group had a significantly shorter healing time than those in the control group: mean(s.d.) 9⋅8(2⋅1) versus 13⋅0(4⋅3) days (P <0⋅001). The Kaplan–Meier median estimate for complete re-epithelialization was 9⋅0 (95 per cent c.i. 8⋅3 to 9⋅7) days in the experimental group, compared with 13⋅0 (12⋅4 to 13⋅6) days in the control group (P <0⋅001) (Fig. 3). Wound healing was quicker in the experimental group in all age groups (P <0⋅050) (data not shown). A greater proportion of patients in the experimental group had healed donor sites by day 14 (51 patients (96 per cent) versus 42 (79 percent) in the control group; P =0⋅008). All donor sites in the experimental group were healed by 3 weeks after surgery, compared with 48 of 53 (91 per cent) in the control group (P =0⋅022).
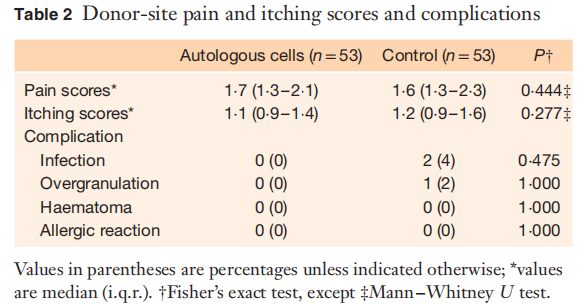
Pain and itching scores are shown in Table 2. Overall pain scores were low (median 1⋅6, i.q.r. 1⋅3–2⋅2), as were itching scores (median 1⋅1, i.q.r. 0⋅9–1⋅5). No significant differences were observed in wound pain or itching scores between the two groups.
There were two donor-site infections, both in the control group (Table 2). Both were superficial infections with redness and swelling, without purulent exudate or positive bacterial cultures; they were treated effectively with povidone–iodine ointment. Overgranulation occurred rarely, and was reported for only one patient in the control group.
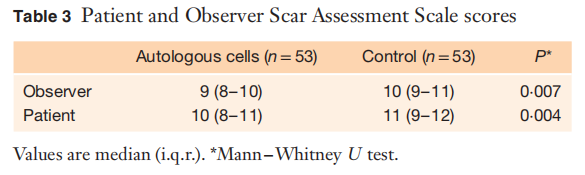
When the quality of donor sites was evaluated at follow-up, those treated with autologous skin cell suspension had better observer and patient scores on POSAS (P =0⋅007 and P =0⋅004 respectively) (Table 3).
Discussion
Rapid and effective healing of secondary wounds, such as skin graft donor sites, is an important consideration in any reconstructive procedure. The present trial assessed autologous skin cell suspension for skin graft donor sites, and showed significantly quicker re-epithelialization and a higher proportion of healed donor sites compared with control treatment. Donor sites receiving autologous skin cell suspension also had better physical attributes, and greater patient satisfaction with healing quality. The autologous skin cell suspension treatment seemed to be safe, without any complications.
Median time to healing was 9⋅0 days in the experimental group, which was quicker than the 13⋅0 days in the control group. Hydrocolloid dressings promote a moist wound environment, and increased collagen synthesis and wound angiogenesis. This environment is also optimal for skin cell proliferation5,6. Autologous skin cell suspension enables delivery of viable keratinocytes, fibroblasts, melanocytes and Langerhans cells harvested from a small STSG sample for application across the wound surface15. In addition, basal layer cells, extracted from the basal lamina, are known to have stem cell-like characteristics22,26, and may be important contributors to the clinical benefit derived from the cell suspension.
Guerid and colleagues14 reported a randomized trial of 45 patients who were treated with autologous keratinocyte suspension in a platelet concentrate, with a mean healing time of 5⋅7 days. Campanella and co-workers23 compared a silicone dressing and a monofilament polyamide woven dressing on paediatric donor sites treated with autologous skin cells, with equivalent rates of epithelialization. No other comparative study of autologous skin cell suspension using hydrocolloid dressings has been undertaken. In the present study, complete re-epithelialization was defined by the covering of all affected areas without any persisting scabs, and assessed by blinded review of the wound image and view of the actual wound. Although wound assessment is subjective, with the possibility of interobserver variation, it was considered to be a feasible and reliable method of measuring wound closure27,28.
Pain, itching and discomfort at the donor site are a significant issue, and methods to alleviate this are an important consideration. Overall pain and itching scores were low in this study and comparable to those reported by Brölmann et al.5. It was expected that postoperative pain and itching would be reduced in the experimental group, but there were no significant differences in pain scores, indicating no meaningful difference for the patients.
The cosmetic appearance of donor sites was assessed after 12 weeks. The POSAS score is a reliable and valid instrument for identifying changes in scar characteristics23,25. The donor sites receiving autologous skin cell suspension displayed better physical attributes and patients were more satisfied with healing quality. Early and rapid re-epithelialization is thought to enhance wound healing and improve long-term aesthetic appearance. In addition, the harvesting and transfer of melanocytes likely contributes to the appropriate pigmentation20,21.
There were some limitations to this study. The single-centre design may decrease external validity, but the generous inclusion criteria, comprising all adults requiring a split-skin graft for any indication, allowed application to a broad patient population. The trial was not double-blind, but bias was minimized by using an independent plastic surgeon and expert in wound care blinded to allocated treatment to view the actual wound and to review wound photographs pertaining to the primary endpoint.
Autologous skin cell suspension technology is frequently used for acute and chronic wounds as an adjunct to standard skin grafting procedures22. The autologous skin cell suspension is produced quickly and is available immediately for wound application. This study suggests that its use as a skin graft donor should promote healing and improve long-term aesthetic results.
Acknowledgements
Z.H., D.G. and J.Z. contributed equally to this study. The authors thank Y. Zhang for support in randomizing patients and statistical analyses. This work was supported by grants from the National Natural Science Foundation of China (81571908, 81272096, 81471875 and 81501675), the Guangdong Provincial Natural Science Foundation (2014A030313099), the Guangzhou City Science and Technology Programme (1561000117) and the Sun Yat-sen University Clinical Research 5010 Programme (2013001). Disclosure: The authors declare no conflict of interest.
References
1. Singh M, Nuutila K, Kruse C, Robson MC, Caterson E, Eriksson E. Challenging the conventional therapy: emerging skin graft techniques for wound healing. Plast Reconstr Surg 2015; 136: 524e–530e.
2. Llanos S, Danilla S, Barraza C, Armijo E, Piñeros JL, Quintas M et al. Effectiveness of negative pressure closure in the integration of split thickness skin grafts: a randomized, double-masked, controlled trial. Ann Surg 2006; 244: 700–705.
3. Akan M, Yildirim S, Misirlio˘glu A, Ulusoy G, Aköz T, Avci G. An alternative method to minimize pain in the split-thickness skin graft donor site. Plast Reconstr Surg 2003; 111: 2243–2249.
4. Dornseifer U, Lonic D, Gerstung TI, Herter F, Fichter AM, Holm C et al. The ideal split-thickness skin graft donor-site dressing: a clinical comparative trial of a modified polyurethane dressing and aquacel. Plast Reconstr Surg 2011; 128: 918–924.
5. Brölmann FE, Eskes AM, Goslings JC, Niessen FB, de Bree R, Vahl AC et al. Randomized clinical trial of donor-site wound dressings after split-skin grafting. Br J Surg 2013; 100: 619–627.
6. Wiechula R. The use of moist wound-healing dressings in the management of split-thickness skin graft donor sites: a systematic review. Int J Nurs Pract 2003; 9: S9–S17.
7. Erba P, Ogawa R, Ackermann M, Adini A, Miele LF, Dastouri P et al. Angiogenesis in wounds treated by microdeformational wound therapy. Ann Surg 2011; 253: 402–409.
8. Prather JL, Tummel EK, Patel AB, Smith DJ, Gould LJ. Prospective randomized controlled trial comparing the effects of noncontact low-frequency ultrasound with standard care in healing split-thickness donor sites. J Am Coll Surg 2015; 221: 309–318.
9. Ottomann C, Hartmann B, Tyler J, Maier H, Thiele R, Schaden W et al. Prospective randomized trial of accelerated re-epithelization of skin graft donor sites using extracorporeal shock wave therapy. J Am Coll Surg 2010; 211: 361–367.
10. Hata K. Current issues regarding skin substitutes using living cells as industrial materials. J Artif Organs 2007; 10: 129–132.
11. Castilla DM, Liu ZJ, Tian R, Li Y, Livingstone AS, Velazquez OC. A novel autologous cell-based therapy to promote diabetic wound healing. Ann Surg 2012; 256: 560–572.
12. Kao HK, Chen B, Murphy GF, Li Q, Orgill DP, Guo L. Peripheral blood fibrocytes: enhancement of wound healing by cell proliferation, re-epithelialization, contraction, and angiogenesis. Ann Surg 2011; 254: 1066–1074.
13. Vanscheidt W, Ukat A, Horak V, Brüning H, Hunyadi J, Pavlicek R et al. Treatment of recalcitrant venous leg ulcers with autologous keratinocytes in fibrin sealant: a multinational randomized controlled clinical trial. Wound Repair Regen 2007; 15: 308–315.
14. Guerid S, Darwiche SE, Berger MM, Applegate LA, Benathan M, Raffoul W. Autologous keratinocyte suspension in platelet concentrate accelerates and enhances wound healing – a prospective randomized clinical trial on skin graft donor sites: platelet concentrate and keratinocytes on donor sites. Fibrogenesis Tissue Repair 2013; 6: 1–8.
15. Wood FM, Giles N, Stevenson A, Rea S, Fear M. Characterisation of the cell suspension harvested from the dermal epidermal junction using a ReCell® kit. Burns 2012; 38: 44–51.
16. Barrandon Y, Green H. Three clonal types of keratinocyte with different capacities for multiplication. Proc Natl Acad Sci USA 1987; 84: 2302–2306.
17. Wood F, Martin L, Lewis D, Rawlins J, McWilliams T, Burrows S et al. A prospective randomised clinical pilot study to compare the effectiveness of Biobrane® synthetic wound dressing, with or without autologous cell suspension, to the local standard treatment regimen in paediatric scald injuries. Burns 2012; 38: 830–839.
18. Gravante G, Di Fede MC, Araco A, Grimaldi M, De Angelis B, Arpino A et al. A randomized trial comparing ReCell system of epidermal cells delivery versus classic skin grafts for the treatment of deep partial thickness burns. Burns 2007; 33: 966–972.
19. De Angelis B, Migner A, Lucarini L, Agovino A, Cervelli V. The use of a non cultured autologous cell suspension to repair chronic ulcers. Int Wound J 2015; 12: 32–39.
20. Mulekar SV, Ghwish B, Al Issa A, Al Eisa A. Treatment of vitiligo lesions by ReCell vs. conventional melanocyte– keratinocyte transplantation: a pilot study. Br J Dermatol 2008; 158: 45–49.
21. O’Neill TB, Rawlins J, Rea S, Wood F. Treatment of a large congenital melanocytic nevus with dermabrasion and autologous cell suspension (ReCELL®): a case report. J Plast Reconstr Aesthet Surg 2011; 64: 1672–1676.
22. Hu ZC, Chen D, Guo D, Liang YY, Zhang J, Zhu JY et al. Randomized clinical trial of autologous skin cell suspension combined with skin grafting for chronic wounds. Br J Surg 2015; 102: e117–e123.
23. Campanella SD, Rapley P, Ramelet AS. A randomised controlled pilot study comparing Mepitel® and SurfaSoft® on paediatric donor sites treated with Recell®. Burns 2011; 37: 1334–1342.
24. Meaume S, Perez J, Descamps H, Voinchet V, Jault P, Saunier V et al. Use of a new, flexible lipidocolloid dressing on acute and chronic wounds: results of a clinical study. J Wound Care 2011; 20: 180, 182–185.
25. Draaijers LJ, Tempelman FR, Botman YA, Tuinebreijer WE, Middelkoop E, Kreis RW et al. The Patient and Observer Scar Assessment Scale: a reliable and feasible tool for scar evaluation. Plast Reconstr Surg 2004; 113: 1960–1965.
26. Cotsarelis G, Kaur P, Dhouailly D, Hengge U, Bickenbach J. Epithelial stem cells in the skin: definition, markers, localization and functions. Exp Dermatol 1999; 8: 80–88.
27. Bloemen MC, van Zuijlen PP, Middelkoop E. Reliability of subjective wound assessment. Burns 2011; 37: 566–571.
28. Rennekampff HO, Fimmers R, Metelmann HR, Schumann H, Tenenhaus M. Reliability of photographic analysis of wound epithelialization assessed in human skin graft donor sites and epidermolysis bullosa wounds. Trials 2015; 16: 235.
This article is excerpted from the John Wiley & Sons Ltd by Wound World.

