
Introduction
Type 2 diabetes mellitus (T2DM) has been described as an emerging pandemic, currently affecting over 462 million people worldwide [1]. Equally alarming is the recent increase in prevalence of depression especially during the COVID pandemic, a common mental health disorder which affects approximately 280 million people worldwide [2, 3]. A close link between the two conditions has long been recognised since the seventeenth century, with the famous British physician Thomas Phyllis describing diabetes as “a consequence of prolonged sorrow” [4]. This link has been confirmed by various studies demonstrating that there is an increased prevalence and diagnosis of depression in T2DM patients [5, 6] with one study reporting that T2DM doubles the risk of depression [5]. Conversely, it has also been shown that depression increases the risk of developing diabetes [7, 8] and diabetic complications [9, 10], indicating a bi-directional relationship between the two.
Given the close relationship between diabetes and depression, there has been growing interest to study the modulatory effects of anti-diabetic medications on depression, including novel agents such as dipeptidyl peptidase 4 inhibitor (DPP4I) and sodium-glucose co-transporter 2 inhibitor (SGLT2I). While early case reports suggested a potential association between incretin-based therapies and depression [11, 12], recent cohort studies have found that DPP4I use is generally associated with a reduced risk of depression [13–16]. This is confirmed by clinical findings that DPP4 enzymatic activity is increased in patients with depressive symptoms [17] as well as pre-clinical findings in rodent model that DPP4I use produces antidepressant effects [18,19]. By contrast, there is limited data available to assess the anti-depressant effects of SGLT2I. A cohort study in 2019 found that both DPP4I and SGLT2I were associated with significantly lower risk of depression, but was only based on 1 SGLT2I user [13]. A case report in 2020 described a patient whose depressive symptoms and suicidal ideations resolved after 1 year of SGLT2I initiation [20]. While both showed promising results, it has not been possible to draw any definitive conclusions due to the small sample size of SGLT2I users in the respective studies.
To our knowledge, there has been no large-scale study so far exploring SGLT2I and its association with depression, either in isolation or in a head-to-head comparison with DPP4I. Hence, the aim of this study is to explore the largely unknown association with depression of SGLT2I use as compared against DPP4I, using a large database of Chinese T2DM patients in Hong Kong.
Methods
Ethics approval
This study was approved by the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee (Ethics Committee Approval Number NTEC-2018-0563).
Data sources and study population
This was a retrospective, territory-wide cohort study of T2DM patients in Hong Kong with SGLT2I/DPP4I use between January 1st, 2015, and December 31st, 2019 (Fig. 1). Patients during the aforementioned study period were enrolled and followed up until December 31st, 2019 or until death. Our team has previously used this large dataset for investigating outcomes including atrial fibrillation, stroke, myocardial infarction, heart failure and dementia [21–23].

The patients were identified from the Clinical Data Analysis and Reporting System (CDARS), a territorywide database that centralizes patient information from individual local hospitals to establish a comprehensive set of medical data, including clinical characteristics, disease diagnosis, laboratory results, and drug treatment details. The system has previously been used by both our team and other teams in Hong Kong to conduct epidemiological studies [24–26].
As SGLT2I and DPP4I were only licensed for use in Hong Kong from 2015 onwards, the study is effectively a new user design with all users starting use of the medication during the study period. Patients were followed up from their first use of the medication either until the diagnosis of new-onset depression or until death. Certain patients were excluded from the study cohort, including patients with both DPP4I and SGLT2I use or discontinuation during the study period, without complete demographics data, without mortality data, with pregnancy or gestational diabetes and with prior diagnosis of psychiatric disease of antidepressant exposure. Users of both DPP4I and SGLT2I were excluded to ascertain the effects were due to one of the drugs, as it would be difficult to attribute whether the risk of new-onset depression was due to DPP4I use, SGLT2I use, or a combination of both with or without switching drugs. As drug compliance is not routinely collected within CDARs, users’ compliance to medication is only assessed indirectly through prescription refills.
Clinical and biochemical data were extracted for the present study. Patients' demographics included gender and age of initial drug use (baseline). Prior comorbidities before initial drug use were extracted based on standard International Classification of Diseases Ninth Edition (ICD-9) codes as shown in Supplementary Table 1 and the Charlson comorbidity index was also calculated. Baseline anti-5diabetic medication use, including metformin, sulphonylurea, insulin, acarbose, thiazolidinedione and glucagon-like peptide-1 agonist, was extracted. Baseline laboratory data were also extracted, including complete blood count, biochemical tests, glucose and lipid profiles.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics of patients with SGLT2I and DPP4I use. For baseline clinical characteristics, the continuous variables were presented as mean (standard deviation [SD]) or median (95% confidence interval [CI]/ interquartile range [IQR]), and the categorical variables were presented as total number (percentage). Continuous variables were compared using the two-tailed Mann-Whitney U test, whilst the two-tailed Chi-square test with Yates’ correction was used to test 2 × 2 contingency data. 1:1 propensity score matching between SGLT2I and DPP4I users was performed based on demographics, prior comorbidities and non-SGLT2I/DPP4I medication using the nearestneighbour search strategy with calliper of 0.1. Propensity score matching results between treatment-group (SGLT2I) versus control-group (DPP4I) before and after matching are shown in Supplementary Fig. 1.
Univariate and multivariable Cox regression models were used to identify significant risk predictors for the study outcomes. Regression analysis with one-year lag time, competing risk analysis (cause-specific and sub-distribution models) and different propensity score approaches (propensity score stratification [27], propensity score matching with inverse probability weighting [28] and propensity score matching with stable inverse probability weighting [29]) were also considered. The hazard ratio (HR), 95% CI and P-value were reported. Statistical significance was defined as P-value<0.05. All statistical analyses were performed with RStudio software (Version: 1.1.456), Python (Version: 3.6), and Stata (Version: SE 16.0).
Results
Baseline characteristics before and after propensity score matching
From the 76,147 patients identified on CDARS within the study period, we excluded 17,641 patients including patients with both DPP4I and SGLT2I use or discontinuation during the study period (N =13,251), without complete demographics data (N =17), without mortality data (N =13), with pregnancy or gestational diabetes (N =28), with prior diagnosis of psychiatric disease of antidepressant exposure (N = 4101) and with mortality within 30 days of initial drug exposure (N =231).
After exclusion, the study cohort included 58,506 patients comprising of 19,381 SGLT2I users and 39,125 DPP4I users. The median age was 63.4 years old and 56.10% were male. After a median follow-up duration of 5.56 years [IQR: 5.23–5.8], 1113 (1.90%) patients developed new onset depression including 200(0.34%) SGLT2I users and 913(1.56%) DPP4I users. After 1:1 propensity score matching, the study cohort included 38,762 patients comprising of 19,381 SGLT2I users and 19,381 DPP4I users. 753 (1.94%) patients developed new onset depression including 200 (0.52%) SGLT2I users and 553 (1.43%) DPP4I users. The baseline and clinical characteristics of DPP4I and SGLT2I users before and after propensity score matching are summarized in Table 1. After propensity score matching, most variables showed standardised mean difference (SMD)<0.2, indicating successful matching. The basic and clinical characteristics of patients with/ without new onset depression before and after propensity score matching are summarised in Supplementary Table 2.




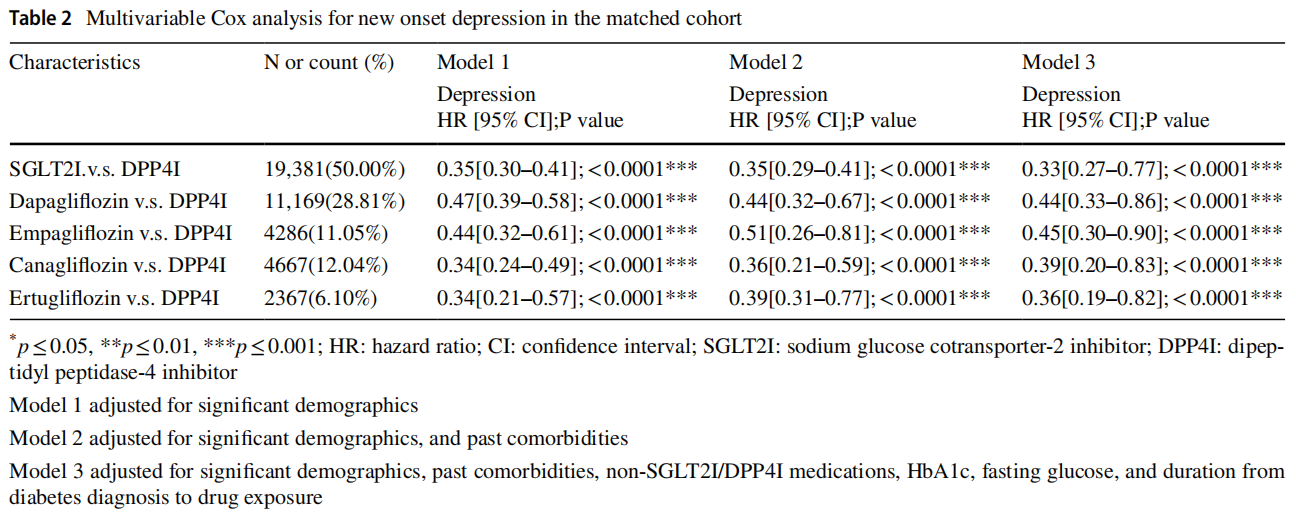
Univariate and multivariable cox regression analyses
Univariate Cox regression models were conducted to identify significant predictors of new-onset depression after 1:1 propensity score matching, as presented in Supplementary Table 3. Compared to DPP4I, SGLT2I use was associated with significantly lower incidence of new onset depression both before (HR: 0.42, 95% CI: [0.36, 0.49], P<0.0001) and after matching (HR: 0.35, 95% CI: [0.30, 0.41], P < 0.0001). Different multivariable Cox regression models adjusting for significant demographics, past co-morbidities, non-SGLT2I/DPP4I medications, HbA1c, fasting glucose and duration of diabetes were performed as presented in Table 2. SGLT2I continued to demonstrate significantly lower association with new onset depression compared to DPP4I after adjusting for the above (HR: 0.33, 95% CI: [0.27, 0.77], P< 0.0001). The cumulative incidence curves for new onset depression in DPP4I and SGLT2I users before and after propensity score matching are presented in Fig. 2.

Sensitivity analysis
Finally, sensitivity analyses for the effects of SGLT2I versus DPP4I use on new onset depression were conducted as presented in Table 3. These included regression analysis with one-year lag time, competing risk analyses using cause specific and sub-distribution hazard models on the matched cohorts and different propensity score-based approaches on the cohort. These analyses confirmed the same findings from the Cox regression models that SGLT2I use is associated with significantly lower incidence of new-onset depression compared to DPP4I use.
Discussion
This key finding of the present study is that SGLT2I users are associated with a lower risk of depression compared to DPP4I users after 1:1 propensity score matching for demographics, prior comorbidities, non-SGLT2I/DPP4I medication use, glycaemic indices and duration of diabetes. This was demonstrated by Cox regression models and further confirmed by competing risk analysis and different propensity score approaches.
Several studies have previously shown that the risk of depression is significantly lowered by DPP4I use in T2DM patients. A prospective study in 2016 of 1735 T2DM patients found that one year of incretin-based therapy use, defined as glucagon-like peptide-1 receptor agonist (GLP1- RA) or DPP4I, was correlated with significant improvement in depressive symptoms as measured by the Patient Health Questionnaire-9 [15]. A UK cohort study in 2018 found that DPP4I use is associated with a lower risk of new-onset depression and self-harm compared to sulphonylurea (HR: 0.80, 95% CI: [0.57, 1.13]) but did not reach statistical threshold [14]. A Japanese cohort study in 2019 of 40,214 patients investigated all classes of anti-diabetic medications and found that only DPP4I use was associated with significantly lower risk for development of depression (HR: 0.31, 95% CI: [0.24, 0.42], P<0.0001) [13]. This has also been confirmed in animal models, such as a study in 2016 demonstrating that sitagliptin has anti-nociceptive and antidepressant effects using a rodent model of depression [18]. Compared to DPP4I, research on the association between SGLT2I and depression has been very limited. The aforementioned 2019 Japanese study is the only study to date to investigate the association between SGLT2I use and depression [13]. The study suggested that SGLT2I use significantly reduces the risk of depression (HR: 0.09, 95% CI: [0.01–0.63], P=0.0153), but was only based on 1 SGLT2I patient and therefore inconclusive.
Multiple studies have demonstrated the neuroprotective effects of SGLT2I, highlighting their potential to improve brain mitochondrial function, hippocampal synaptic plasticity and inhibit acetylcholinesterase [30–33]. It is therefore very possible that SGLT2I exerts its anti-depressant effects via direct effects on the brain. One such mechanism was suggested in a recent study by Muhammad et al. using a rodent model of depression [34]. The neuroimmune hypothesis of depression suggests that mood disorders are mediated by a state of systemic inflammation, defined by activated inflammatory pathways and elevated cytokine levels [35–37]. One such pathway is the nod-like receptor pyrin containing 3 (NLRP3) inflammasome which, when activated in chronic stress, leads to release of pro-inflammatory cytokines such as IL-1β and IL-18 [38]. Muhammad et al. demonstrated that dapagliflozin suppresses NLRP3 inflammasome activation and downstream inflammatory mediators, thus inhibiting neuro-inflammation and blood-brain barrier disturbances. The study also demonstrated that the mechanism of action and efficacy shown by dapagliflozin was analogous, and sometimes superior, to the commonly prescribed anti-depressant Escitalopram [34]. While further studies are required to confirm whether such effects are observed in humans, it gives credence to the exciting anti-depressant potentials of SGLT2I in addition to its main anti-diabetic effects among T2DM patients.
Limitations
Several limitations should be noted for the present study. First, given its observational nature, there is inherent information bias due to under-coding, coding errors and missing data. Secondly, as drug compliance is not routinely collected within CDARS, patient compliance to SGLT2I and DPP4I was only assessed indirectly through prescription refills and was not accounted for in Cox regression analyses. Thirdly, residual and unmeasured confounding may be present despite robust propensity-matching, particularly with the unavailability of information such as patient-level socioeconomic status. Patients’ drug exposure duration has not been controlled, which may affect their risk against the study outcomes.
Conclusion
SGLT2I use is associated with significantly lower risk of depression compared to DPP4 use in patients with type-2 diabetes mellitus using propensity score matching and Cox regression analyses.
Supplementary Information The online version contains supplementary material available at https://doi.org/10.1007/s00592-023-02063-6.
Funding This study was supported by the National Natural Science Foundation of China (NSFC) Grant Nos. 72042018, 71972164, and 71672163, in part by the Health and Medical Research Fund Grant (HMRF), the Food and Health Bureau, the Government of the Hong Kong Special Administrative Region No. 16171991, and in part by the Theme-Based Research Scheme of the Research Grants Council of Hong Kong Grant No. T32-102/14N.
Declarations
Conflicts of interest The authors have no relevant financial or nonfinancial interests to disclose. All authors certify that they have no affiliations with or involvement in any organization or entity with any
financial interest or non-financial interest in the subject matter or ma terials discussed in this manuscript.
Ethical approval This study was approved by the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee (Ethics Committee Approval Number NTEC-2018- 0563).
Informed consent The study does not include identifiable human or animal data requiring consent.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
References
1.Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H,Al KJ (2020) Epidemiology of type 2 diabetes—global burden of disease and forecasted trends. J Epidemiol Glob Health 10(1):107–111
2. Suzuki H, Torigoe K, Numata O, Yazaki S (2000) Infant case with a malignant form of Brugada syndrome. J Cardiovasc Electrophysiol 11(11):1277–1280
3. Santomauro DF, Mantilla Herrera AM, Shadid J et al (2021) Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398(10312):1700–1712
4. Holt RI, de Groot M, Golden SH (2014) Diabetes and depression. Curr Diab Rep 14(6):491
5. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ (2001) The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 24(6):1069–1078
6. Hasan SS, Mamun AA, Clavarino AM, Kairuz T (2015) Incidence and risk of depression associated with diabetes in adults: evidence from longitudinal studies. Commun Ment Health J 51(2):204–210
7. Deleskog A, Ljung R, Forsell Y, Nevriana A, Almas A, Möller J (2019) Severity of depression, anxious distress and the risk of type 2 diabetes—a population-based cohort study in Sweden. BMC Public Health 19(1):1174
8. Campayo A, de Jonge P, Roy JF et al (2010) Depressive disorder and incident diabetes mellitus: the effect of characteristics of depression. Am J Psychiatry 167(5):580–588
9. de Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ (2001) Association of depression and diabetes complications: a meta-analysis. Psychosom Med 63(4):619–630
10. Nouwen A, Adriaanse MC, van Dam K et al (2019) Longitudinal associations between depression and diabetes complications: a systematic review and meta-analysis. Diabet Med 36(12):1562–1572
11. (2008) Sitagliptin: new drug. Type 2 diabetes: limited efficacy, too many unknown risks.Prescrire Int 17(93):12–15
12. Kohen I, Lester P (2008) Exenatide-induced depression in a geriatric patient. Int J Geriatr Psychiatry 23(4):443–444
13. Akimoto H, Tezuka K, Nishida Y, Nakayama T, Takahashi Y, Asai S (2019) Association between use of oral hypoglycemic agents in Japanese patients with type 2 diabetes mellitus and risk of depression: a retrospective cohort study. Pharmacol Res Perspect 7(6):e00536
14. Gamble J-M, Chibrikov E, Midodzi WK, Twells LK, Majumdar SR (2018) Examining the risk of depression or self-harm associated with incretin-based therapies used to manage hyperglycaemia in patients with type 2 diabetes: a cohort study using the UK clinical practice research datalink. BMJ Open 8(10):e023830
15. Moulton CD, Pickup JC, Amiel SA, Winkley K, Ismail K (2016) Investigating incretin-based therapies as a novel treatment for depression in type 2 diabetes: findings from the South London diabetes (SOUL-D) study. Prim Care Diabetes 10(2):156–159
16. Djurovic M, Jemuovic Z, Vasovic O et al (2018) Cognitive status,anxiety and depression in patients with type 2 diabetes mellitus on selective DPP4 inhibitor therapy. Endocr Abstr. https://doi.org/10. 1530/endoabs.56.P498
17. Zheng T, Liu Y, Qin S et al (2016) Increased dipeptidyl peptidase-4 activity is associated with high prevalence of depression in middle-aged and older adults: a cross-sectional study. J Clin Psychiatry 77(10):e1248–e1255
18. Kamble M, Gupta R, Rehan HS, Gupta LK (2016) Neurobehavioral effects of liraglutide and sitagliptin in experimental models. Eur J Pharmacol 774:64–70
19. Saritha MKCK (2018) Antidepressant activity of DPP4-inhibitors in albino mice, an experimental study. Natl J Med Dent Res 6(4):523–526
20. Shimizu ETY, Bando H, Fujita M, Kusaka Y, Yuu M (2020) Effective SGLT2 inhibitor for patient with type 2 diabetes mellitus (T2DM) and depression. Diabetes Res Open Access 2:26–32
21. Mui JV, Zhou J, Lee S et al (2021) Sodium-glucose cotransporter 2 (SGLT2) inhibitors vs. dipeptidyl peptidase-4 (DPP4) inhibitors for new-onset dementia: a propensity score-matched populationbased study with competing risk analysis. Front Cardiovasc Med 8:747620
22. Lee S, Zhou J, Leung KSK et al (2022) Comparison of sodiumglucose cotransporter-2 inhibitor and dipeptidyl peptidase-4 inhibitor on the risks of new-onset atrial fibrillation, stroke and mortality in diabetic patients: a propensity score-matched study in Hong Kong. Cardiovasc Drugs Ther. https://doi.org/10.1007/ s10557-022-07319-x
23. Zhou J, Lee S, Leung KSK et al (2022) Incident heart failure and myocardial infarction in sodium-glucose cotransporter-2 vs. dipeptidyl peptidase-4 inhibitor users. ESC Heart Fail 9(2):1388–1399
24. Lee S, Liu T, Zhou J, Zhang Q, Wong WT, Tse G (2021) Predictions of diabetes complications and mortality using hba1c variability: a 10-year observational cohort study. Acta Diabetol 58(2):171–180
25. Zhou J, Lee S, Guo CL et al (2021) Anticoagulant or antiplatelet use and severe COVID-19 disease: a propensity score-matched territory-wide study. Pharmacol Res 165:105473
26. Zhou J, Wang X, Lee S et al (2020) Proton pump inhibitor or famotidine use and severe COVID-19 disease: a propensity score-matched territory-wide study. Gut. https://doi.org/10.1136/ gutjnl-2020-323668
27. Austin PC (2011) An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res 46(3):399–424
28. Austin PC, Stuart EA (2015) Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med 34(28):3661–3679
29. Avagyan V, Vansteelandt S (2021) Stable inverse probability weighting estimation for longitudinal studies. Scand J Stat 48(3):1046–1067
30. Esterline R, Oscarsson J, Burns J (2020) Chapter Five - A role for sodium glucose cotransporter 2 inhibitors (SGLT2is) in the treatment of Alzheimer’s disease? In: Söderbom G, Esterline R, Oscarsson J, Mattson MP (eds) International review of neurobiology, vol 155. Academic Press, Cambridge, pp 113–140
31. Sa-Nguanmoo P, Tanajak P, Kerdphoo S et al (2017) SGLT2-inhibitor and DPP-4 inhibitor improve brain function via attenuating mitochondrial dysfunction, insulin resistance, inflammation, and apoptosis in HFD-induced obese rats. Toxicol Appl Pharmacol 333:43–50
32. Wiciński M, Wódkiewicz E, Górski K, Walczak M, Malinowski B (2020) Perspective of SGLT2 inhibition in treatment of conditions connected to neuronal loss: focus on Alzheimer’s disease and ischemia-related brain injury. Pharmaceuticals 13(11):379
33. Lin B, Koibuchi N, Hasegawa Y et al (2014) Glycemic control with empagliflozin, a novel selective SGLT2 inhibitor, ameliorates cardiovascular injury and cognitive dysfunction in obese and type 2 diabetic mice. Cardiovasc Diabetol 13:148
34. Muhammad RN, Ahmed LA, Abdul Salam RM, Ahmed KA, Attia AS (2021) Crosstalk among NLRP3 inflammasome, ETBR signaling, and miRNAs in stress-induced depression-like behavior: a modulatory role for SGLT2 inhibitors. Neurotherapeutics. https:// doi.org/10.1007/s13311-021-01140-4
35. Ménard C, Hodes GE, Russo SJ (2016) Pathogenesis of depression: Insights from human and rodent studies. Neuroscience 321:138–162
36. Pitsillou E, Bresnehan SM, Kagarakis EA et al (2020) The cellular and molecular basis of major depressive disorder: towards a unified model for understanding clinical depression. Mol Biol Rep 47(1):753–770
37. Wei L, Li Y, Tang W et al (2019) Chronic unpredictable mild stress in rats induces colonic inflammation. Front Physiol 10:1228
38. Kaufmann FN, Costa AP, Ghisleni G et al (2017) NLRP3 inflammasome-driven pathways in depression: clinical and preclinical findings. Brain Behav Immun 64:367–383
Publisher's Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is excerpted from the Acta Diabetologica (2023) 60:917–927 by Wound World.

