糖尿病足?
根据糖尿病这个基础疾病,合并不愈合的足部伤口,大多数人首先想到糖尿病足!
分享一个案例:
-
男性患者,81岁,左足背红肿疼痛2月。既往有2型糖尿病、高血压病史多年。
-
患者2月前足背出现破溃,就诊当地医院,予清除+局部换药+封闭式负压引流治疗,仍未愈合。
-
查体:负压引流后

-
辅助检查:糖化血红蛋白 7.4%,肌酐 125mmol/L,尿酸509umol/L,左下肢动脉彩超提示动脉硬化,胫前后、足背动脉阶段性轻度狭窄。
初步诊断:
-
左侧2型糖尿病足溃疡
-
慢性肾功能不全(氮质血症期)
-
2型糖尿病
-
高血压病
-
高尿酸血症
治疗:控制血糖、改善循环、局部负压引流
肉芽红润,伤口不愈合;红肿消了,为啥剧烈疼痛呢?
 再次局部切开,发现了白色物质
再次局部切开,发现了白色物质

-
高度怀疑痛风石,导致的足部溃疡、疼痛、阻碍愈合! 什么检查,可以确诊是痛风石引起的疼痛呢? 就是双能CT,绿色部分为痛风石:

报告:
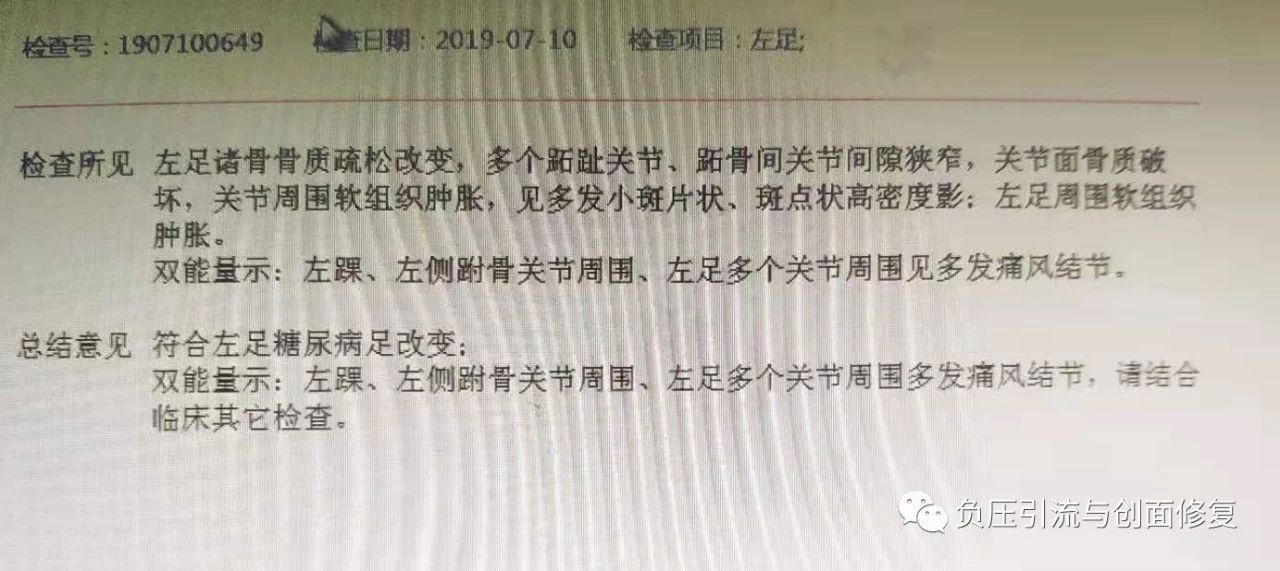
修正诊断:左足痛风性结节并破溃
调整治疗方案:
-
局部改普通换药:痛风性伤口,使用负压引流,无效果;
-
管好嘴:
-
加用降尿酸药物:对于已形成痛风性关节炎、痛风结石的患者,需要药物来协助溶解关节内的痛风石,然后通过尿液排出。代表药物有苯溴马隆、别嘌呤醇片、非布司他片等;
-
补充益生菌:体内物质的吸收、合成、分解、排泄与肠道内的益生菌关节密切,补充“益生菌”的思路是直接吃进活的细菌类似于空投一些“好细菌”来抑制“坏细菌”;
-
多喝水

