
斑秃是非瘢痕性脱发,现在认为是T淋巴细胞活化介导的自身免疫性疾病!,有自愈倾向。虽然本病不会危及生命,但对患者造成较大的精神痛苦和心理压力。有研究显示,微针有刺激毛发生长的作用[]。本研究对1例斑秃患者采用单纯微针治疗,达到满意效果。
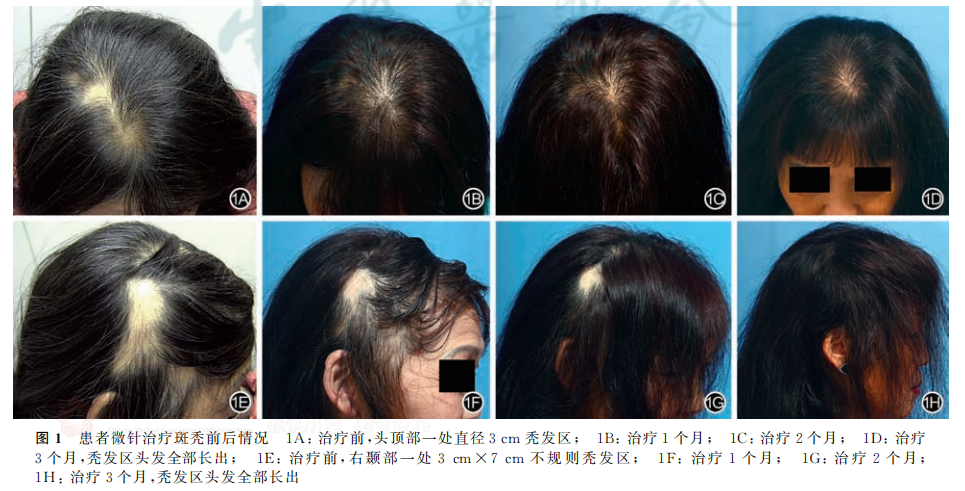
病例 患者,女,58岁。因多发性斑块状脱发12个月余来杭州市第一人民医院整形外科门诊就诊。患者自觉近12个月来头发脱落较严重,以斑状脱发为主。曾接受过曲安奈德皮损内注射、局部糖皮质激素乳音、5%米诺地尔洗剂治疗,均未见明显改善。患者一般情况较好,睡眠质量较差,有高血压病史半年,口服苯磺酸氨氯地平片,一日1片,血压控制可;有焦虑症病史。无家族遗传性脱发史。相关检查:除抗核抗体弱阳性外,甲状腺功能、IgE均正常,真菌镜检阴性、梅毒螺旋体抗体检测阴性。头皮组织病理检查提示毛囊周围轻度炎症细胞浸润,浸润细胞以淋巴细胞为主,有少量嗜酸粒细胞和肥大细胞;可见毛囊微小化及营养不良毛囊。整形外科检查:患者头顶部一处直径3cm秃发区、右题部一处3cmx7cm不规则秃发区;拉发试验阳性。皮肤镜检查可见题部秃发区毛发稀少,毳毛偶见;头顶部秃发区有较多毳毛,可见黄点征、猪尾样毛发和直立性再生发。患者头顶部在治疗过程中再次出现直径约1cm大小的类圆形脱发斑的秃发斑。
治疗经过:我们仅用微针治疗秃发区,每两周1次,共治疗3个月。每次治疗调节微针(一次性使用皮肤点刺针,苏州美沃思医疗科技有限公司),长度1.5mm。治疗前,于患者秃发区外用利多卡因乳音,40min后用生理盐水擦拭和乙醇消毒治疗区3遍:操作者在相同力度下对头皮秃发区反复施针3遍,直至患者头皮出现微红或散在出血点。治疗结束,再用乙醇消毒。嘱患者治疗当天禁止洗头。治疗过程无痛,治疗期间或治疗后均无明显不良反应。每次微针治疗后,患者脱发明显改善。毛发镜下显示,毛发密度、毛囊密度、平均直径、终毛占比和毳毛占比均显著改善。患者定期随访3个月,毛发生长良好,脱发斑块已不可见,且无复发见图 1。
讨论
越来越多的证据显示,微针治疗斑秃有效果。Chandrashekar 等!研究显示,2例斑秃头顶和额头出现秃发区,分别持续6个月和12个月,且曲安奈德皮损内注射、局部糖皮质激素乳膏和5%米诺地尔洗剂治疗无效,用微针联合局部曲安奈德治疗 3次(每隔 3周)后,秃发区毛发再生长,随访3个月斑秃未复发。为排除斑秃自愈的可能,本例患者斑秃处于进展期,病程较长,且各种治疗方法均无效,我们观察到,每次治疗后秃发区及毛发稀疏部位均表现出明显地改善,说明微针可促进斑秃患者毛发再生。
利益冲突 所有作者均声明不存在利益冲突
参 考 文 献
[1]陈军生,何洁冰,魏旷荣,等.斑秃患者血 T 细胞变化及其凋亡信号控制[J].中华医学美学美容杂志,2002,8(1):23-26.DOl:10,3760/cma.j.issn.1671-0290.2002.01.008.
[2]施辛,马维祥.斑秃患者抑郁情绪研究[J].中华医学美学美容杂志,2004,10(4):242-243.DOI:10.3760/cma.j.issn.16710290.2004.04.024.
[3] Kim YS, Jeong KH, Kim JE, et al. Repeated microneedlestimulation induces enhanced hair growth in a murine model[]Ann Dermatol,2016,28(5):586-592. DO1:10.5021/ad.2016.28.5.586. Epub 2016 Sep 30.
[4]Chandrashekar B, YepuriV, Mysore V. Alopecia areata-suc-cessful outcome with microneedling and triamcinolone acetonide[J].JCutan Aesthet Surg, 2014,7(1):63-64. DOI:10.4103/0974-2077.129989.
本文献转载于中华医学美学美容杂志2023年4月第29卷第2期,不代表本网站赞同其观点和对其真实性负责,我们主要用于阅读分享,非商业用途,如若侵权,请告知删除。

