











This article is excerpted from the Pharmacology & Therapeutics 260 (2024) 108681 by Wound World.
Anna Nicolaou a,b, ⁎, Alexandra C. Kendall a
a Laboratory for Lipidomics and Lipid Biology, Division of Pharmacy and Optometry, School of Health Sciences, Faculty of Biology Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester M13 9NT, UK
b Lydia Becker Institute of Immunology and Inflammation; Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester M13 9NT, UK
article info
Available online 17 June 2024
Associate editor: Dr. M. Curtis
Keywords:
Skin barrier
Microbiota
Bioactive lipids
Ceramides
Skin disease
Skin immunology
abstract
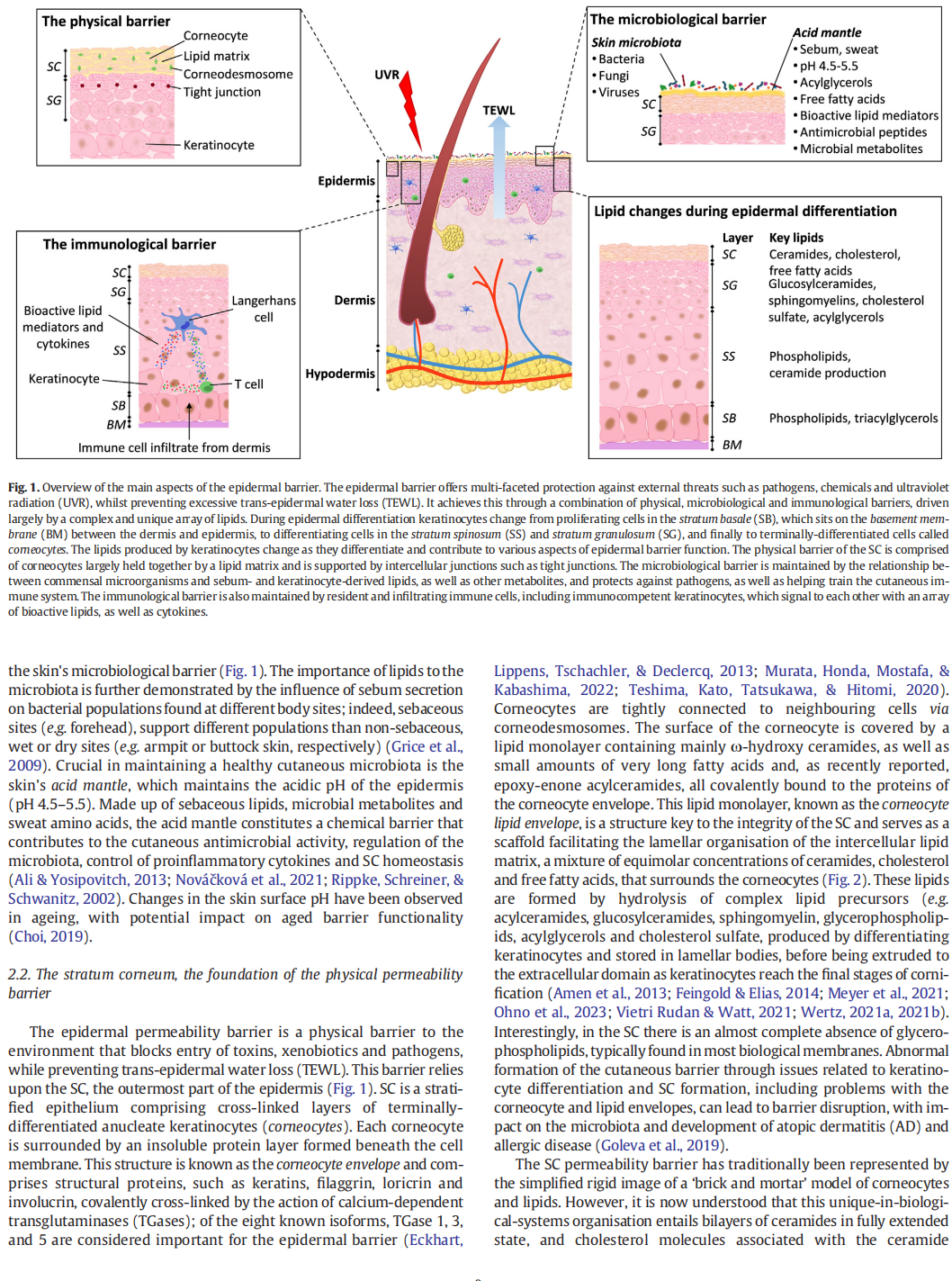
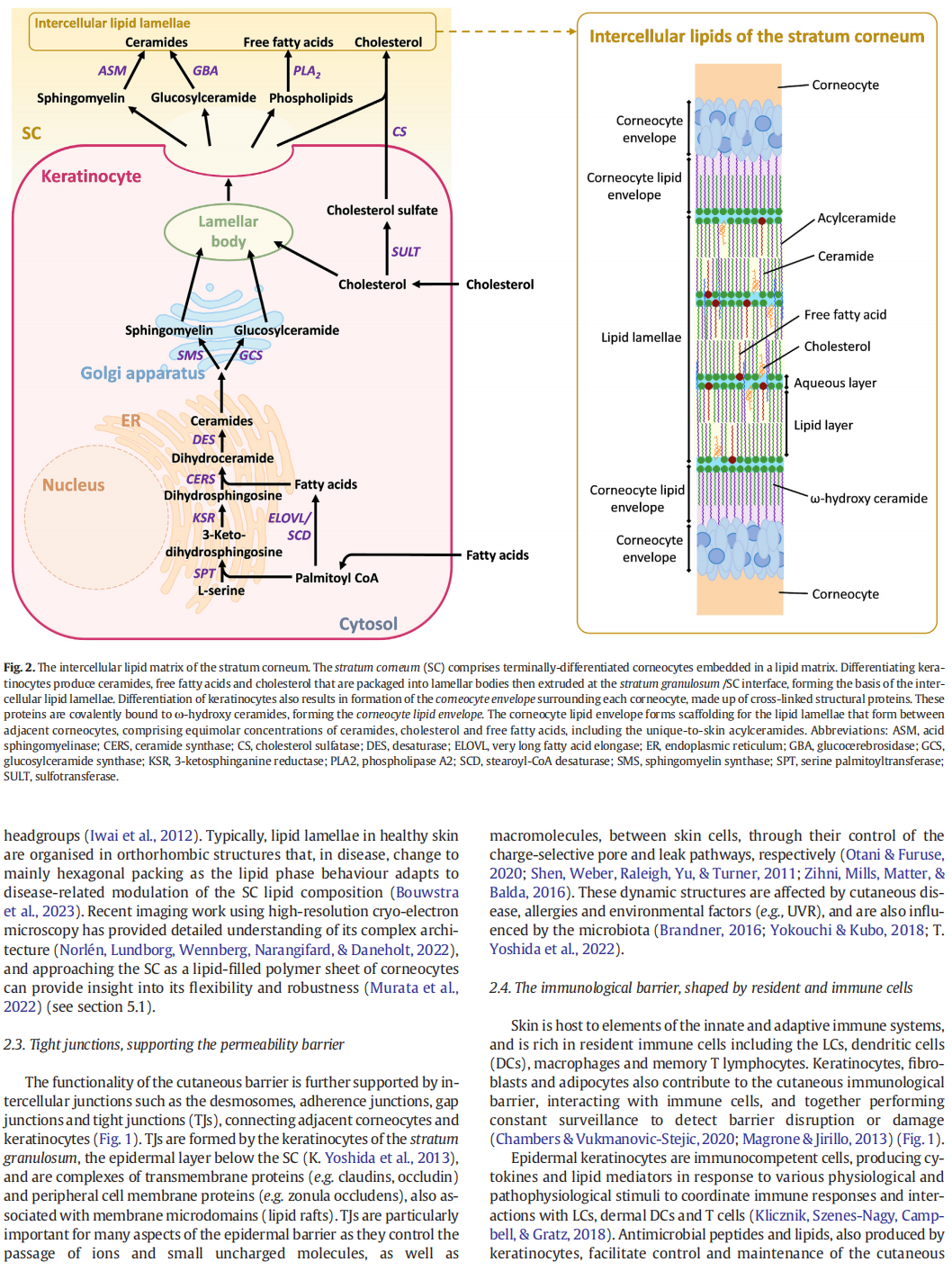
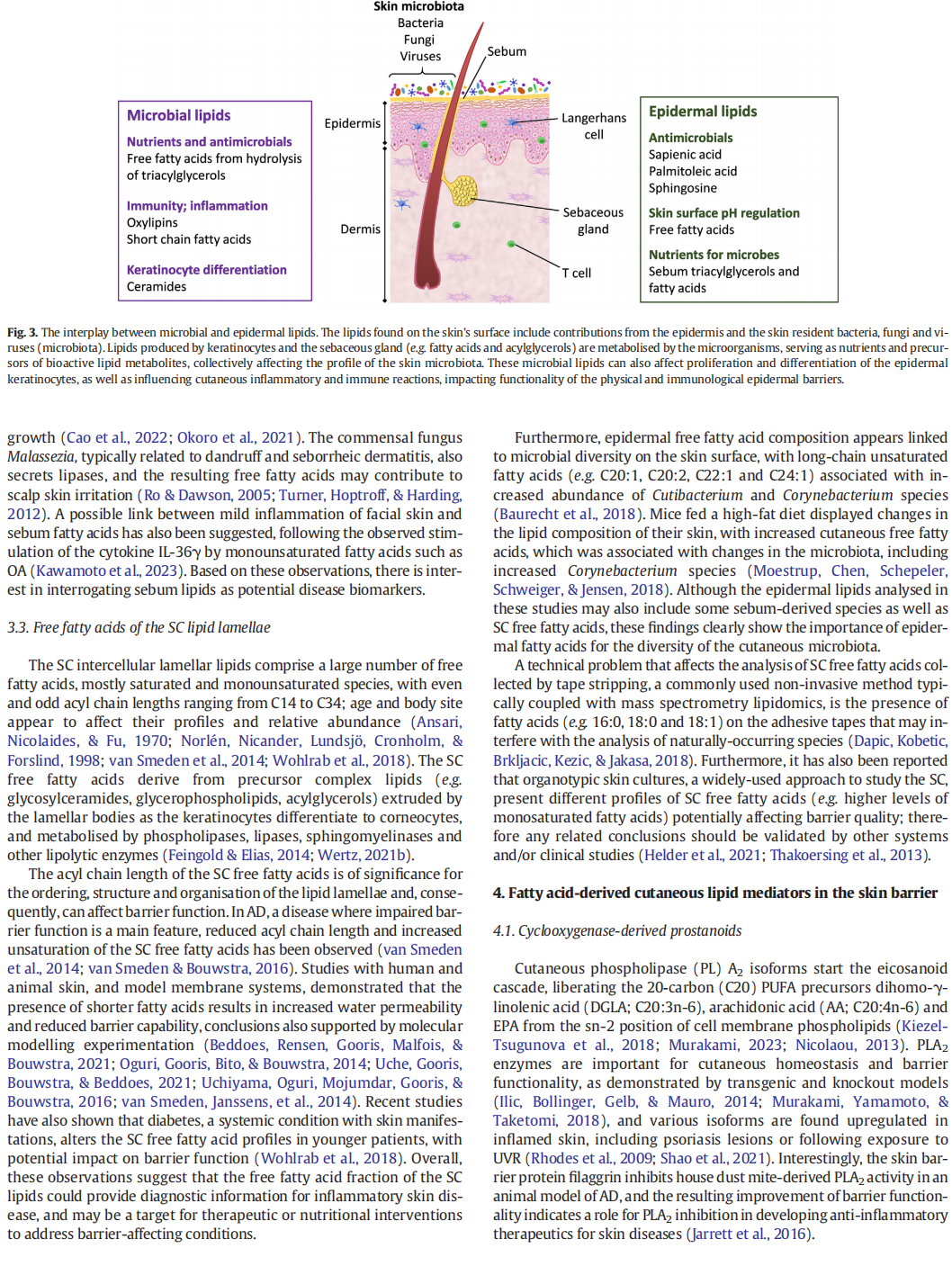
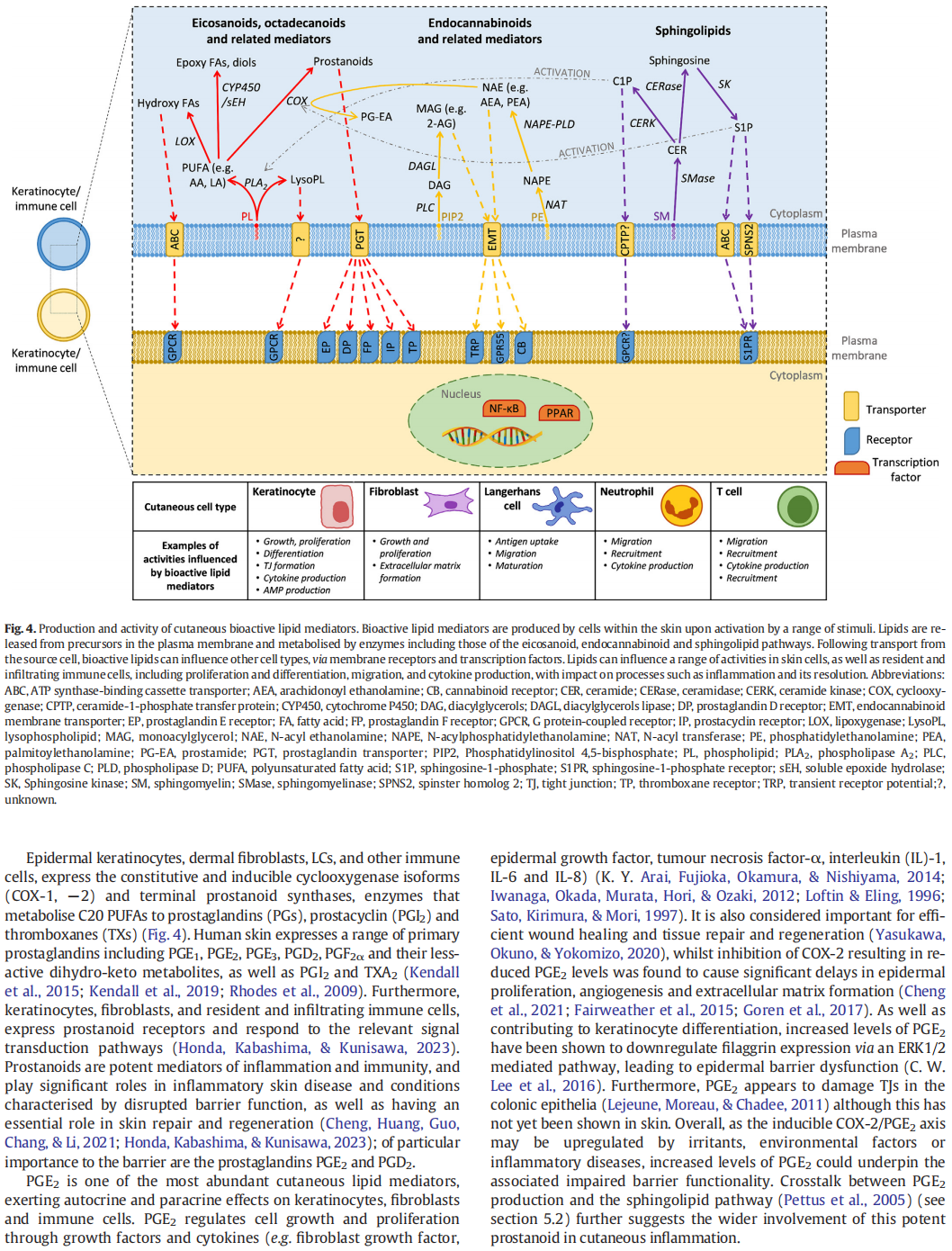
Our skin protects us from external threats including ultraviolet radiation, pathogens and chemicals, and prevents excessive trans-epidermal water loss. These varied activities are reliant on a vast array of lipids, many of which are unique to skin, and that support physical, microbiological and immunological barriers. The cutaneous physical barrier is dependent on a specific lipid matrix that surrounds terminally-differentiated keratinocytes in the stratum corneum. Sebum- and keratinocyte-derived lipids cover the skin's surface and support and regulate the skin microbiota. Meanwhile, lipids signal between resident and infiltrating cutaneous immune cells, driving in-flammation and its resolution in response to pathogens and other threats. Lipids of particular importance include ceramides, which are crucial for stratum corneum lipid matrix formation and therefore physical barrier functionality, fatty acids, which contribute to the acidic pH of the skin surface and regulate the microbiota, as well as the stratum corneum lipid matrix, and bioactive metabolites of these fatty acids, involved in cell signalling, inflammation, and numerous other cutaneous processes. These diverse and complex lipids maintain homeostasis in healthy skin, and are implicated in many cutaneous diseases, as well as unrelated systemic conditions with skin manifestations, and processes such as ageing. Lipids also contribute to the gut-skin axis, signalling between the two barrier sites. Therefore, skin lipids provide a valuable resource for exploration of healthy cutaneous processes, local and systemic disease development and progression, and accessible biomarker discovery for systemic disease, as well as an opportunity to fully understand the relationship between the host and the skin microbiota. Investigation of skin lipids could provide diagnostic and prognostic biomarkers, and help identify new targets for interventions. Development and improvement of existing in vitro and in silico approaches to explore the cutaneous lipidome, as well as advances in skin lipidomics technologies, will facilitate ongoing progress in skin lipid research.
© 2024 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
Abbreviations: ASM, Acid sphingomyelinase; ALA, α-linolenic acid; AA, arachidonic acid; AEA, arachidonoyl ethanolamine; AG, arachidonoyl glycerol; AD, atopic dermatitis; BM, basement membrane; CerS, ceramide synthase; CLA, conjugated linoleic acid; COX, cyclooxygenase; CYP450, cytochrome P450 monooxygenase; DC, dendritic cell; DGAT, diacylglycerol acyltransferase; DGLA, dihomo-γ-linolenic acid; DHA, docosahexaenoic acid; DHEA, docosahexaenoyl ethanolamine; EPA, eicosapentaenoic acid; EPA, eicosapentaenoyl ethanolamine; EV, extracellular vesicles; FATP, fatty acid transfer protein; GBA, glucocerebrosidase; GCS, glucosylceramide synthase; PC, phosphatidylcholine; HYA, 10-hydroxy cis-10-octadecanoid acid; HETE, hydroxyeicosatetraenoic acid; HODE, hydroxyoctadecaenoic acid; LC, Langerhans cell; LA, linoleic acid; LOX, lipoxygenase; LC-MS/MS, liquid chromatography coupled to tandem mass spectrometry; LPA, lysophosphatidic acid; MAG, monoacylglycerol; NSAID, non-steroidal anti-inflammatory drug; NAE, N-acyl ethanolamine; OA, oleic acid; OEA, oleoyl ethanolamine; n-3, omega-3; n-6, omega-6; C1P, phosphorylated ceramide; PEA, palmitoyl ethanolamine; PNPLA1, patatin-like phospholipase domain-containing protein 1; PPAR, peroxisome proliferator-activated receptor; PAF, platelet activating factor; PUFA, polyunsaturated fatty acid; PGI2, prostacyclin; PG, prostaglandin; SCFA, short chain fatty acid; SPT, serine palmitoyl transferase; DEGS, sphingolipid desaturase; SMS, sphingomyelin synthase; S1P, sphingosine-1-phosphate; SEA, stearoyl ethanolamine; SB, stratum basale; SC, stratum corneum; SG, stratum granulosum; SS, stratum spinosum; TX, thromboxane; TJ, tight junction; TEWL, trans-epidermal water loss; TGase, transglutaminase; Tri-HOME, trihydroxy octadecenoic acid; UVR, ultraviolet radiation; ELOVL., very long fatty acid elongase.
⁎ Corresponding author at: Division of Pharmacy and Optometry, Stopford Building, Oxford Road, University of Manchester, Manchester M13 9PT, UK.
E-mail address: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。 (A. Nicolaou).
This article is excerpted from the Pharmacology & Therapeutics 260 (2024) 108681 by Wound World.

