
伤口世界
- 星期一, 19 9月 2022
Conductive Biomaterials as Bioactive Wound Dressing for Wound Healing and Skin Tissue Engineering(2)
4. 3D Conductive Biomaterials for Wound Healing
2D conductive biomaterials have made great achievement in wound healing. Through adopting multiple functions, they can promote cell attachment, proliferation, differentiation, and further the whole wound healing process. However, they are still restrained on thin and superficial wounds. In contrast, 3D biomaterials such as hydrogels, foams, and sponges possessing high water absorbance capacity can deal with wounds with high exudate [67]. On the other hand, deep wounds and chronic wounds have poor regenerative capacity due to versatile mechanism, such as lack of cell sources, severe infection, limited blood supply, immunosuppression or immunodeficiency, metabolic diseases, and other environmental factors [13]. Fortunately, 3D biomaterials possessing ECM-mimicking architecture could be utilized as scaffolds for these issues, which could not only support the integrity of dermis, but also act as carriers for bioactive reagents and cells [63].
4.1 Hydrogel
Due to the porous 3D interconnected structure and highwater content, hydrogel owns a lot of advantages as wound dressing [35, 145, 169]. Hydrogel allows oxygen and water vapor to pass through, maintains a humid environment, lowers the wound temperature, and relieves pain [170]. The soft nature, flexibility, and stretchability support hydrogel being compliant with human skin under ceaseless movement [171, 172]. Moreover, hydrogel has great tolerance to integrate multiple functions, including mechanical properties and additional therapeutic effects [173]. Correspondingly, hydrogel wound dressings have attracted most intensive attention in the past few years. Recently developed conductive hydro- gel-based wound dressings are summarized in Table 3.
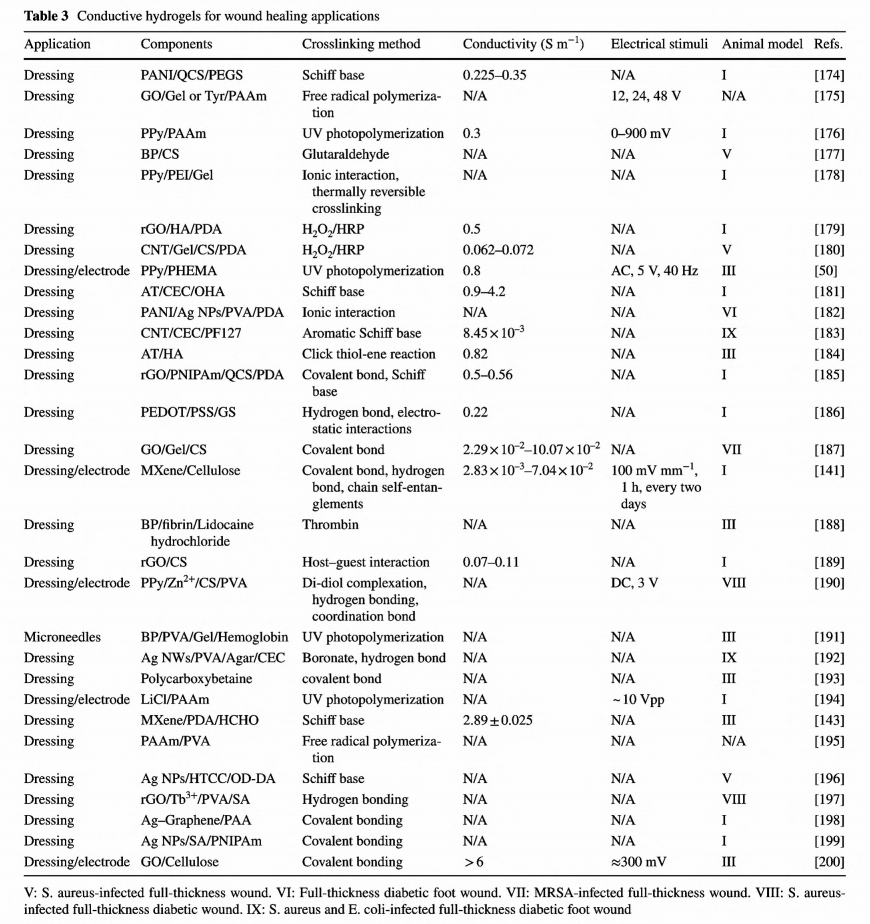
So far, versatile conductive hydrogels with different conductive components have been developed. In contrast to most 2D biomaterials-based wound dressings which validate their potential in wound dressing by in vitro cell culture assay, the wound healing efficacy of most conductive hydrogels has been proved both by in vitro and in vivo animal assays. However, unlike the situations of film wound dressings where electrical activities of conductive substances can be isolated to prove their effects on cellular activities, the wound healing performance is always enhanced through synergistic effects from electrical activities, antioxidant, and antibacterial activities of hydrogel-based wound dressings. In 2015, Hsiao et al. synthesized a chitosan derivate with self- doped PANI which could form colloidal gels induced by pH increase and explored the photothermal antibacterial activities in vitro and on subcutaneous abscess [201]. But the conductivity and the electroactivity were not examined in this work. Since then, these relevant features of the conductive substances were comprehensively evaluated via standard protocols. Our group has designed multifunctional conductive hydrogel-based wound dressings and proven their positive performance in accelerating wound healing process [165, 179 -181, 183, 185, 187]. Chitosan, a natural polysaccharide, has been utilized in wound dressing for a long time, owing to its inherent antibacterial, analgesic effect and hemostatic activity [202]. However, the poor solubility of chitosan under neutral and constrained antibacterial effectiveness under nonacidic environments extremely limit its application and efficacy of wound healing. Fortunately, the abundant active amino groups enable further modification. Quaternized chitosan (QCS) is a better choice for its excellent antibacterial activities and improved solubility. Our group not only solves the above issues, but also broadens its derivates and applications as wound dressing.
As shown in Fig. 8, quaternized chitosan-g-polyaniline (QCSP) synthesized and demonstrated good water solubility and enhanced antibacterial activity and biocompatibility than pure chitosan [203]. Meanwhile, the residue active amino groups remained potential to react with other groups. In this work, QCSP was then crosslinked with benzaldehyde group functionalized poly (ethylene glycol)-Co-poly (glycerol sebacate) via Schiff base forming the hydrogel network [174]. The optimal hydrogel dressing showed an ionic conductivity of 2.37 mS cm-1 that is close to that of human dermis, thus owning the ability to transfer bioelectrical signals for accelerating wound healing. Overall, com- pared with Tegaderm™ film, the optimal hydrogel dressing performed excellent enhanced wound healing covering all stages, including in vivo blood clotting capacity, promoted ECM synthesis, collagen deposition, granulation tissue thickness, and promoted remolding phase. We also developed a supramolecular conductive hydrogel based on QCS and graphene oxide graft-cyclodextrin [189]. The dynamic host-guest interactions were employed as crosslinkers endowing the hydrogel with self- healing and injectability. Considering the antibacterial activity, cell proliferation, and hemocompatibility, the hydrogel with 0.4 wt% of rGO was selected as the optimal dressing. Indeed, this conductive hydrogel dressing exhibited enhanced wound healing on full-thickness wounds. It is worthy to mention that , we validated that Pluronic F127 and polydopamine are of great advantages in designing carbon nanomaterials incorporated hydrogels, including assisting homogeneous dispersion, improving mechanical properties and tissue adhesiveness [183, 185].
In addition, conductive hydrogels can promote the efficiency of electrotherapy. Commonly in clinic, small metal electrodes were attached on human body near the wounds; thus, ES could not directly cover the whole wound [194]. As the large impedance of human skin, it is only possible to apply ES on every inch of wounds under high voltage, which may threat more danger to the patients [24, 204]. In scientific research, conductive films and fabrics have been justified to promote wound healing under ES for covering the whole wound bed [42, 115, 155, 157]. Reasonably, conductive hydrogel is another good choice, in terms of conductivity, softness, stretchability, and flexibility. Recently, a conductive hydrogel containing poly(2-hydroxyethyl methacrylate) and PPy has justified superior to commercial hydrogel dressing considering the antibacterial capacity and alleviated secondary damage during removal. Moreover, the significance of this work was that the replacement of traditional separate electrodes with one integral conductive hydrogel can extremely promote the efficacy of electrotherapy [50]. Zhang et al. created a conductive hydrogel using Zn2+ and PPy as the conductive components and chitosan as the main polymer backbone. This hydrogel was capable of sensing temperature and strain variations and accelerating the infected chronic wounds with ES [190]. More impressively, Jeong et al. developed an ionic hydrogel dressing based on LiCl and combined the dressing with a prototypical wearable triboelectric nanogenerator [194]. The nanogenerator can harvest biophysical energy from friction between skin and deliver ES to hydrogel, while the hydrogel dressing directly distributes ES to the whole wound.
Another attractive feature of hydrogel biomaterial is the great potential in tissue engineering by acting as scaffold to support cells and biomolecules. Mesenchymal stem cell combined with an ECM- mimicking biomaterial has attracted much attention in chronic wound healing [205- 207]. Conductive hydrogel has been employed as scaffold for the treatment of diabetic wounds. Jin et al. recently reported a conductive hydrogel scaffold based on AT, hyaluronic acid and gelatin [184]. Compared with nonconductive hydrogel, the conductive hydrogel was found to upregulate the level of Cx43, owing to better transport of molecules and ions between cells. What's even more impressive, O2-consuming enzyme laccase was introduced to cast a hypoxic microenvironment, and this hypoxic environment could maintain for almost 12 h. Furthermoe, adipose-derived mesenchymal stem cells were loaded for direct delivery to the hostile wound, while relative cell activity remained higher than 85% within 2 days. Thus, this conductive hydrogel could act as a multifunctional scaffold for chronic wounds. Overall, conductive hydrogels could promote wound healing process via diversiform approaches, thus being regarded as valuable candidates for wound healing, particularly for complicated chronic wounds. On the other hand, the excellent conductivity, easy fabrication method, and facile surface modification enable conductive hydrogels with great potential in health care devices for wound diagnosis. But , the long-term durability of hydrogel may impede this progress.
4.2 Fibrous Scaffold
Even though electrospun scaffolds have been reckoned as promising candidates for tissue engineering, their applications still constrained by several factors, such as pore size and pore interconnectivity that all affect cellular infiltration and tissue ingrowth into the scaffold. Small pore size did not hinder the application for nanofibers as wound dressing, but cell attachment and proliferation might be restrained on the surface of nanofibers [162, 1 64]. Nanofibers with too compact structures could not fulfill the requirements of porous scaffolds for tissue engineering applications [208]. A nonwoven conductive web composed of PEDOT and PLLA was fabricated by melt-spinning. After culture for 48 h, human dermal fibroblasts appeared throughout the scaffold, indicating the web permitted cell infiltration [156]. Another interesting work is about a polyaniline-multi-walled carbon nanotube/PNIPAm composite electrospun nanofibers-based “smart”scaffold with temperature responsiveness for cell delivery [159]. Above LCST, this conductive nanofibrous
scaffolds demonstrated enhanced fibroblast attachment and proliferation, while below LCST, the encapsulated cells would detach and been delivered to human body. Moreover, this stimuli-responsive nanofiber network was inflammation-sensitive, and can deal with loco-regional acidosis, which helps to pass through the inflammation phase. Therefore, conductive nanofibrous scaffold could be envisioned with great value in skin tissue engineering with deliberate design.
4.3 Sponge, Foam, and Acellular Dermal Matrix
Hydrogel-derived aerogel and cryogel have sponge-like structures and high polarity for water absorption and thus could not only manage with a large amount of water, but also permit water to flow out/in freely [209- 213]. Foam also has an interconnected porous structure and is commonly manufactured from polyurethane or silicone [9, 15]. Without further modifications with a hydrophilic surface, the pure foam demonstrates hydrophobicity, thus benefiting inherent antibacterial properties [33]. The subtle difference between sponge and foam is that foam usually exhibited more enhanced mechanical properties than sponge [33]. Generally, foam and sponge dressings can be used for various types of wounds, including burn, ulcer, skin donor area, and transplant. Also, they are lightweight, elastic, and easy to use in practice. As the second layer of skin, the dermis consists of a connective ECM with fibroblasts, endothelial cells, smooth muscle cells, and mast cells [214, 215]. ECM supports the main structure of skin tissue, develops interactions with versatile growth factors, and modulates cellular activities [63]. Acellular dermal matrix (ADM) derived from human or animal skin has been widely used in tissue engineering and wound healing as tissue replacement, graft and wound dressing [216, 217] The currently developed 3D conductive wound dressings are listed in Table 4.
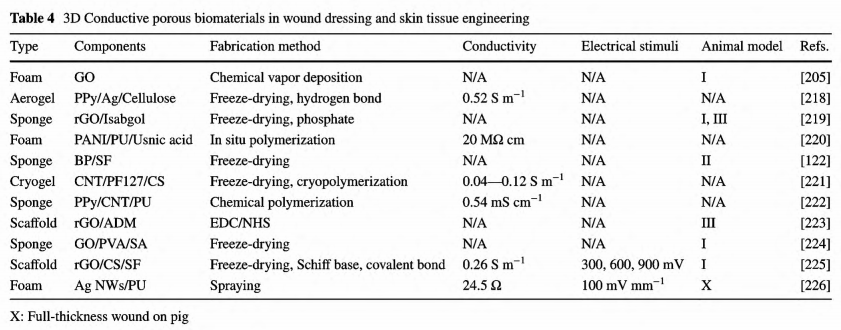
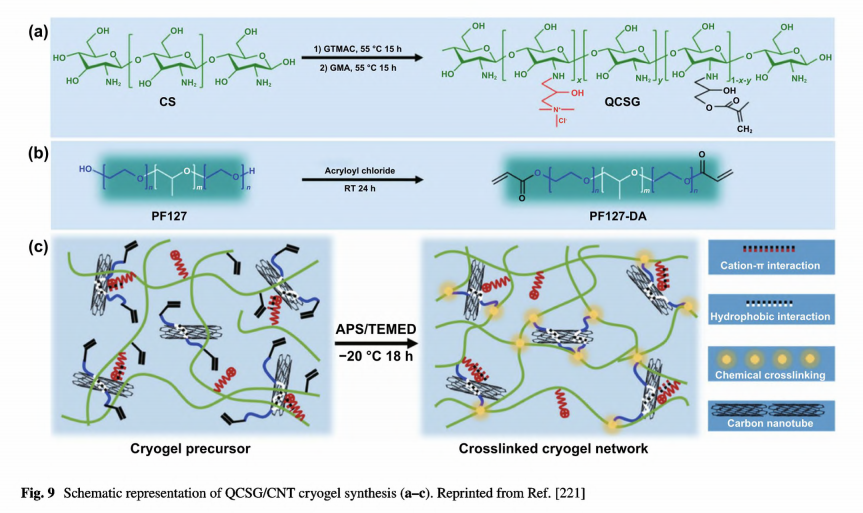
Our group developed a conductive cryogel composed of chitosan and PF127- assisted homodispersed CNT, while CNT providing conductivity and reinforcement toward the mechanical properties, as shown in Fig. 9 [221]. Com- pared with cryogel from pure natural polymers, commercial gelatin hemostatic sponge, and Combat Gauze, this CNT hybrid cryogel (QCSG/CNT) demonstrated rapid blood- triggered shape recovery and absorption speed, high blood uptake capacity, and hemostatic capability. Moreover, CNT provided this cryogel with photothermal effect and NIR- assisted photothermal antibacterial activity. Compared with commercial Tegaderm™ film and nonconductive cryogel, the conductive cryogel demonstrated better wound healing performance with the least inflammatory infiltration, and the highest vascularization by 15 days.
The ADM comprised of extracellular matrix proteins and collagen demonstrates excellent biocompatibility, suitable mechanical properties, and bioactivity which is ideal for skin tissue scaffold. Fu et al. developed a rGO incorporated ADM-based scaffold via simple solution immersion process in which ADM was crosslinked with EDC and NHS [223]. The topology and structural integrity preserved after loading with rGO. Compared with the primitive scaffold and scaffold loaded with GO, ADM-rGO demonstrated superior cell attachment and proliferation for mesenchymal stem cells and human skin fibroblasts. Eventually, acting as a transplanting platform for mesenchymal stem ells, this conductive scaffold demonstrated enhanced therapeutic effect toward diabetic wounds. Based on the above, 3D conductive biomaterials have demonstrated encouraging results in promoting loaded with GO, ADM-rGO demonstrated superior cell attachment and proliferation for mesenchymal stem cells and human skin fibroblasts. Eventually, acting as a transplanting platform for mesenchymal stem cells, this conductive scaffold demonstrated enhanced therapeutic effect toward diabetic wounds. Based on the above, 3D conductive biomaterials have demonstrated encouraging results in promoting wound healing by working as wound dressings.
3D conductive biomaterials demonstrate promising potential in electrodes for electrotherapy and scaffolds for skin tissue engineering. Chen et al. reported an Ag nanowiresloaded foam demonstrating flexibility, enhanced conductivity, and long-term stability under physiological environment [226]. Due to the inherent antibacterial activity, good water-uptake capability, and electrical conductivity, the conductive foam could not only prevent infection and manage necrosis, but also implement annular oriented electrical field to wounds assisted by exogenous electrical fields. In the in vivo experiment on full-thickness pig skin wound, compared with control group treated with gauze, wounds treated with the conductive foam absent from exogenous electrical fields demonstrated enhanced wound healing performance for smaller wound residual area, controlled inflammation, better neovascularization, and advanced re- epithelialization. More excitingly, when applying the conductive foam with exogenous electrical fields, wounds demonstrated the most superior wound healing effect and therefore proved the great value of 3D conductive biomaterials in wound dressing, as well as their application in electrotherapy. Furthermore, the intrinsic feature of the highly porous structure enabled this conductive foam to connect with negative-pressure drainage closure device, thus simultaneously promote the wound healing process. Especially, since the structure, composition, appendages, and healing mechanism of porcine skin are closer to human skin, these results are more convincing.
5. Application of Conductive Biomaterials in Wound Healing
Regardless of different types of the wounds, the healing process occurs in a similar systematic manner including four distinct phases, as illustrated in Fig.10 [227]. Ideally, hemostasis occurs immediately after injury and would complete within seconds or hours depending on wound size, depth, and wound location. Then, inflammation begins and lasts for several days and reaches the highest level by 72 h. The third phase, proliferation is more complicated. Angiogenesis, fibroblast migration, granulation tissue formation, collagen deposition, epithelialization, and wound contraction take place simultaneously. Finally, the last remodeling phase allowing granulation tissue to develop into mature connective tissue may last for several months to years. With standard wound care, acute wounds can progress through the healing routine steadily. However, in practice, normal wound healing would be affected and disrupted by many factors, including nutrition, oxygen supply, infection, aging, chronic disease, wound treatment, and even genetics. Extensive tissue damage, necrotic debris, and diseases often make wounds suffer from such issues, thus leading to prolonged inflammation and delayed proliferation and remodeling. Wound with delayed healing more than 3 months would be referred to as chronic wound [10, 228, 229]. In detail, chronic wounds with impaired regenerative capacity demonstrate high levels of proinflammatory cytokines, persistent infections, and drug resistance. Apparently, chronic wounds need specific treatment including tissue debridement, infection clearance, moisture balance, mechanical support, and management of comorbidities according to the etiology and real-time diagnosis.

Wound dressings and skin tissue scaffolds are of great importance in wound care and skin tissue regeneration [27,160]. There have been developed plenty commercial products to fulfill the requirements for different wounds. Biomaterials with specific functions have also been symmetrically studied in promoting wound healing, such as antibacterial, hemostatic, adhesive, injectable, and antioxidant property. Conductive biomaterials demonstrate promising potential in wound healing as well, because they could regulate and promote cell attachment and relevant activities with or without ES that have been convinced by in vitro and in vivo assays [44, 61, 230]. So far, researchers have successfully validated the effectiveness of conductive biomaterials in different types of wounds, both for acute and chronic wounds. Moreover, due to the intrinsic electroconductivity, conductive wound dressings can be applied in real-time diagnosis. It is worth mentioning that conductive biomaterials are usually combined with other bioactive substances to meet the requirements in practice.
5.1 Acute Wound
An acute wound is an unintentional injury to skin that can be caused by surgical incisions, bites, deep lacerations, abrasions, and burns [2, 3, 11, 33]. Acute wounds can spontaneously heal in an orderly routine even without any external intervention. In scientific research, clean incisional and excisional wounds with controlled area and facile surgery are frequently utilized to evaluate the effectiveness of wound dressings. Generally, a full-thickness wound with clear edge is created by surgical incision on the back of rat or pig. Full- thickness wound means a loss of all layers of the skin and great potential of the exposure of underlying tissues. Deep infection and fluid exudate affect the healing process, as well [15]. To address such issues, conductive biomaterials-based wound dressings integrating multiple functions are of high needs.
5.1.1 2D Conductive Biomaterials for Acute Wound
As incisional and excisional wounds on rat or pig skin have light exudate, 2D biomaterial-based wound dressings can meet the requirements of wound care. Conductive film, membrane, and nanofibers have all realized their applications in acute full-thickness wounds. CPs and oligomers incorporated biomaterials have obtained great attention for their facile synthesis. In 2015, Gharibi et al. developed a series of polyurethane/siloxane-based conductive wound dressing containing aniline tetramer moieties [148]. These wound membranes displayed electroactivity, antimicrobial activity, and antioxidant ability which could promote fibroblast growth and proliferation. Besides, these CSA-doped membranes revealed comparable equilibrium water absorption value and water vapor transmission rate to some commercially available dressings, and suitable surface hydrophilicity to support cellular activity. Thus, the authors suggested these membranes could work as wound dressings for acute and chronic wounds, because the above three parameters are important to evaluate whether a product could maintain a moist environment for wounds. In an in vivo animal assay last for 20 days, the designed membranes exhibited accelerated wound healing than commercial cotton gauze. Our group synthesized a conductive polyurethane film, in which PCL provided mechanical properties, PEG contributed to surface wettability and AT supported electroactivity [118]. Through in vitro and in vivo assays, the conductive film with 12% AT content revealed improved cell adhesion and proliferation, and enhanced wound healing performance than nonelectroactive commercial dressing. Recently, our group also proved the viability of conductive nanofibers as wound dressing in practice. The electroactive nanofibers were electrospun from PCL and QCSP, thus demonstrating suitable mechanical properties, electroactivity and antibacterial properties [165]. The microporous structure can not only support cellular activities, but also guarantee the nanofibers to absorb exudate from wounds. The balance between antibacterial activity and cell proliferation should be taken into consideration as well, for bilateral properties of QCSP. Eventually, the conductive nanofibers with 15 wt% of QCSP were selected as the optimum dressings. Indeed, compared with Tegaderm™ film, the electroactive nanofibers exhibited improved wound healing efficiency with rapid wound contraction, higher collagen depostion, lower production of TGF-a, and higher expression of VEGF within 14 days.
Except for the antibacterial activities, metals and metal oxides can generate ES under specific conditions. Liu et al. utilized template- assisted magnetron sputtering method to modify commercial spunlace cotton nonwovens with metal dots (Ag, Zn), as shown in Fig. 11 [120]. The low content of metals enabled the dressing with good cytocompatibility. Interestingly, this conductive Ag/Zn@Cotton dressing demonstrated enhanced cell migration and accelerated wound healing, which was attributed to the generation of ES and inherent antibacterial activities of Ag t/Zn2+ with continuous release under moist conditions. Bhang et al. developed a piezoelectric dermal patch based on zinc oxide nanorod and applied this patch in treating full-thickness wounds [115]. Under small mechanical deformations, this patch generated electrical fields. In animal assay, the patch was found to promote wound healing process via a series of cellular activities, including inflammation regulation, cell proliferation, re-epithelization, angiogenic factor secretion, and tissue remodeling.

In common, to address complications in acute wounds, 2D conductive biomaterials always need to be endowed with multiple bioactive functions while fulfilling basic requirements. However, the application of 2D conductive biomaterials in acute wound healing is still restricted by some parameters, such as the limited capacity for managing exudate, loading bioactive agents and maintaining their biological activities, further functionalization, and low adhesion to skin.
The literature is to be continued……
This article is excerpted from the Nano-Micro Letters by Wound World.
- 星期五, 16 9月 2022
Conductive Biomaterials as Bioactive Wound Dressing for Wound Healing and Skin Tissue Engineering(1)
RuiYu1, HualeiZhang1,2, BaolinGuo1,2
Baolin Guo, baoling@ mail.xjtu.edu.cn
State Key Laboratory for Mechanical Behavior of Materials, and Frontier Institute of Science and Technology, Xi' an Jiaotong University,Xi'an 710049, People's Republic of China
Key Laboratory of Shaanxi Province for Craniofacial Precision Medicine Research, College of Stomatology, Xi'an Jiaotong University,Xi'an 710049, People's Republic of China
Published online: 02 December 2021
HIGHLIGHTS
●The design and application of conductive biomaterials for wound healing are comprehensively reviewed, including versatile conductive agents, the various forms of conductive wound dressings, and different in vivo applications.
●Three main strategies of which conductive biomaterials realizing their applications in wound healing and skin tissue engineering are discussed.
●The challenges and perspectives in designing multifunctional conductive biomaterials and further clinical translation are proposed.
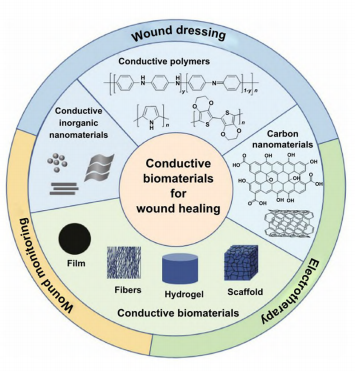
ABSTRACT Conductive biomaterials based on conductive polymers, carbon nanomaterials, or conductive inorganic nanomaterials demonstrate great potential in wound healing and skin tissue engineering, owing to the similar conductivity to human skin, good antioxidant and antibacterial activities, electrically controlled drug delivery, and photothermal effect. However, a review highlights the design and application of conductive biomaterials for wound healing and skin tissue engineering is lacking. In this review, the design and fabrication methods of conductive biomaterials with various structural forms including film, nanofiber, membrane, hydrogel, sponge, foam, and acellular dermal matrix for applications in wound healing and skin tissue engineering and the corresponding mechanism in promoting the healing process were summarized. The approaches that conductive biomaterials realize their great value in healing wounds via three main strategies (electrotherapy, wound dressing, and wound assessment) were reviewed. The application of conductive biomaterials as wound dressing when facing different wounds including acute wound and chronic wound (infected wound and diabetic wound) and for wound monitoring is discussed in detail. The challenges and perspectives in designing and developing multifunctional conductive biomaterials are proposed as well.
KEYWORDS Conducting polymers; Inorganic nanomaterials; Biomaterials; Electrotherapy; Wound monitoring
Cite as
Nano-Micro Lett. (2022) 14:1
Received: 29 July 2021
Acepted: 29 October 2021 ◎The Author(s) 2021

- 星期三, 14 9月 2022
应用功能材料促进皮肤创面修复
罗高兴 刘梦龙
陆军军医大学(第三军医大学)第一附属医院全军烧伤研究所,创伤、烧伤与复合伤国家重点实验室,重庆市疾病蛋白质组学重点实验室 400038
通信作者:罗高兴 Email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
【摘要】皮肤创面是临床常见病症之一。功能材料通过结构调节和性能整合,可以针对性地对创面进行保护并促进创面愈合,目前已在创面修复领域得到广泛应用,是临床创面治疗的重要工具之一。本文分别就止血类、抗菌类、抗炎类、促血管化类及调控创面微环境类功能材料在创面修复中的应用做一总结。
【关键词】皮肤;伤口愈合;功能材料;创面微环境
基金项目: 国家自然科学基金重点国际合作项目(81920108022);国家自然科学基金重点项目(81630055)
Application of functional materials to promote cutaneous wound healing
Luo Gaoxing, Liu Menglong
State Key Laboratory of Trauma, Burns and Combined Injury, Institute of Burn Research, the First Affiliated Hospital of Army Medical University (the Third Military Medical University), Chongqing Key Laboratory for Disease Proteomics, Chongqing 400038, China Corresponding author: Luo Gaoxing, Email: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
[ Abstract ] Cutaneous wound is one of the common clinical diseases. Functional materials can provide targeted wound protection and promote wound healing through the structural adjustment and functional integration. Currently, functional materials have been widely used in the field of wound repair, becoming one of the important tools for clinical wound treatment. This paper summarizes the application of functional
materials of following categories including hemostasis,antibacterial, anti-inflammation, vascularization, and regulation of wound microenvironment in wound repair.
[ Key words ] Skin; W ound healing; Functional materials; W ound microenvironment
Fund program: Key International Cooperation Program of National Natural Science Foundation of China (81920108022); Key Program of N ational Natural Science Foundation of China (81630055).
- 星期二, 13 9月 2022
利用表皮干细胞治疗兔角膜缘干细胞缺损
金 岩F! 刘 源 *! 张 超*! 董 蕊*! 雷 娟*
(第四军医大学组织工程研发中心, 西安 710032
摘要: 目 的 利 用 自 体 表 皮 干 细 胞 与 异 体 角 膜 基 质 细 胞 在 体 外 构 建 双 层 组 织 工 程 角 膜 ! 并 修 复 兔 角 膜 缘 干 细 胞 的 缺 损 " 方 法 建 立 兔 角 膜 缘 干 细 胞 缺 损 模 型 ! 以 去 细 胞 猪 角 膜 基 质 片 作 为 支 架 材 料 ! 以 自 体 表 皮 干 细 胞 与 异 体 角 膜 基 质 细 胞 作 为 种 子 细 胞 ! 在 体 外 构 建 组 织 工 程 角 膜 ! 并 用 来 修 复 兔 角 膜 缘 干 细 胞 缺 损 " 结 果 利 用 自 体 表皮 干 细 胞 与 异 体角 膜 基 质 细 胞 复合 异 种 去 角 膜 基 质 片 在 体 外 成 功 构 建 组 织 工 程 角 膜 # 构 建 的 组 织 工 程 角 膜 与 正 常 角膜 相 似 ! 具 有 上 皮层 和 基 质 层 # 用 组 织 工 程 角 膜 修 复 兔 角 膜 缘 干 细 胞 缺 损 T 个 月 后 ! 损 伤 角 膜 透 明 度 恢 复 良 好 ! 组 织 学 结 构基 本 恢 复 正 常 " 结论 成 功 构 建 了 兔 的双 层 组 织 工 程 眼角 膜 ! 并 修 复 了 兔角 膜 缘 干 细 胞 缺损 "
关键词" 表皮干细胞# 角膜# 组织工程# 角膜损伤
中图分类号:R 775.2
文献标识码:2
文章编号: 1000-503X(2005)06-0674-04
Treatment of Rabbit Corneal W ounds with Skin Epidermal Stem Cells
Jin Yan*, Liu Yuan*, Zhang Chao*, Dong Rui*, Lei Juan*
(Research Center for Tissue Engineering, the Fourth Military Medical University, Xi'an 710032, China)
Abstract: Objective To construct artificial rabbit corneas with autologous skin epidermal stem cells and allogenic stromal cells in vitro and promote healing of corneal wounds.
Methods: Skin epidermal stem cells were isolated from autologous skin samples. Keratocytes were isolated from newborn cornea biopsies. The cells were combined with acelular porcine corneal stroma scaffold to construct artificial corneas. Then the constructed artificial corneas were used to repair severe vision loss caused by complete loss of corneal epithelial stem cells.
Results: Cultured skin epidermal stem cells and keratocytes were in good growth conditions.Cultured artificial corneas consisted of multiplayer epithelial cells growing on stroma equivalent consisting of stromal matrix with incorporated keratocytes. The in vitro constructed artificial corneas were histologically similar to normal rabbit corneas. Three months after transplantation, the cornea wounds were healed and the rabbit cornea became transparent.
Conclusion: The artificial corneas were constructed successfully in vitro and can be used to repair severe vision loss caused by complete loss of corneal epithelial stem cells.
Key words: epidermal stem cells; cornea; tissue engineering; comeal wound Acta Acad Med Sin, 2005 ,27(6):674-677
Acta Acad Med Sin, 2005 ,27(6):674-677
- 星期五, 09 9月 2022
Metabolic surgery in China: present and future
Yinfang Tu", Yuqian Bao回1,2*, and Pin Zhang 3,*
1 Department of Endocrinology and Metabolism, Shanghai Jiao Tong University Affiliated Sixth People's Hospital Shanghai Diabetes Institute, Shanghai Clinical Center of Diabetes, Shanghai Key Laboratory of Diabetes Mellitus, Shanghai Key Clinical Center for Metabolic Disease, Shanghai 200233, China
2 Department of Endocrinology and Metabolism, jinshan District Central Hospital of Shanghai Sixth People's Hospital, Shanghai 201 599, China
3 Department of Bariatric and Metabolic Surgery, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai 200233, China* Correspondence to: Yuqian Bao, E-mail: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。; Pin Zhang, E-mail: 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
Edited by Wei-Ping Jia
Obesity and its related complications comprise a serious public health problem worldwide, and obesity is increasing in China.
Metabolic surgery is a new type of treatment with unique advantages in weight loss and obesity-related metabolic complications.
The pathogenesis of obesity is complex and not yet fully understood. Here, we review the current efficacy and safety of metabolic surgery, as well as recent progress in mechanistic studies and surgical procedures in China. The exciting and rapid advances in this field provide new opportunities for patients with obesity and strike a balance between long-term effectiveness and safety.
Keywords: metabolic surgery, type 2 diabetes mellitus, obesity, metabolic syndrome.
Received March 14, 2021. Revised May 27, 2021. Accepted June 14, 2021.
◎The Author(s) (2021). Published by Oxford University Press on behalf of Journal of Molecular Cell Biology, CEMCS, CAS.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http:/ /creativecommons.org/ licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals. 该Email地址已收到反垃圾邮件插件保护。要显示它您需要在浏览器中启用JavaScript。
- 星期四, 08 9月 2022
大鼠自体异体表皮细胞悬液混合移植 的实验研究
吕国忠 朱宇刚 周红梅 顾在秋 杨敏杰
[摘要]
目的探讨自.异体表皮细胞悬液混合移植技术在创而修复中的应用、
方法 30只,大鼠随机配成15对后.分成细胞悬液移植组(A组,10对)和细胞膜片移植组(B组,5对)。取每只大鼠的去全厚皮创面分离表皮细胞,并根据配对情况按1:1的细胞比例混合,体外常规培养。4 d后收获A组混合细胞悬液,14 d后收获B组混介细胞膜片、将此细胞悬液和膜片分别转移至A、B组相应供体大鼠的去全厚皮创面、随后A组每对大鼠的创面交叉覆益配对方的体全厚皮;B组创血覆盖胶原膜及“优妥”敷料。比较移梢后2~3周两组的创面修复情况。
结果 术后2~3 尚,A组创面大多愈介,表面光滑.与皮下连接紧密。术后第5天,B组创面部分细胞膜片脱落,部分成活。膜片成活的
创面后期再次出现小创面经久不愈,
结论 自异体表皮细胞悬液混合移植足一种可行的、体内构建皮肤、修复创面的方法。
[关键词] 表皮;细胞培养; 皮肤移植;烧伤
An experimental study on the in vivo intermingled culture of rat autologous and allogeneic epithelial cells LV Cuozhong, ZHU Yugang, ZHOU Hongmei. Department of Burns, The Third People' s Hospital, Wuxi 214041,Jiangsu Province, P. R. China
[ Abstract] Objective To explore a method for in vivo skin reconstruction. Methods Thirty Spraque-Dawley ( SD) rats were randomly divided into two paired groups, i. e. in vivo culture ( A group,10
pairs) and in vitro grafting (B group,5 pairs). Skin samples were harvested from the rats of the two groups for the isolation of epithelial cells which were then mixed cultured in vitro in 1: I ratio. Mixed cellular sus- pension in A group was harvested 4 days after culture. The mixed cellular sheets were harvested 14 days after culture. The cultured cells and sheets were then thansplanted onto ttal skin loss wounds of donor rats for further cultivation. The wounds in A group were covered with allogeneic full-thickness skin. While the wounds in group were covered by collagen membrane and gauze. Wound repair was observed and compared between the two groups al 2-3 post - operative weeks.
Results
Most of the wounds in A group healed after 2-3 weeks with smooth surface, and the peithelium connected closely and tightly with the: subcutaneous tissue. In the wounds in B group on 5 post-operative day . some of the cellular sheets survived and some fell off. Even the healed wounds in B group would be injured again resulting in protracted small wounds.
Conclusion In vivo in situ epithelia! culture might be an optional method of skin reconstruction for wound healing.
[Key words] Epithelium; Cell culture; Skin graft; Burm

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}